Normally the brain's cells communicate with other cells by firing tiny electrical signals. Sometimes something goes wrong, and the cells signal many times faster than normal. That abnormal signaling causes an attack called a seizure. Seizures usually include sudden, abnormal movements and behaviors. People who have had two or more seizures have a condition called epilepsy.
Symptoms
The main symptom, or sign, of epilepsy is the seizure. There are two types of seizures: generalized and partial. Generalized seizures result from abnormal signals in most of the brain. Partial seizures result from abnormal signals in part of the brain.
During a generalized seizure the person may fall down and lose consciousness. The muscles may jerk, turn stiff, or become limp for a few minutes. Breathing can stop temporarily. After a violent seizure the person feels confused and tired. In some cases a generalized seizure is hard to notice. The person may just lose consciousness for a few seconds and stare or blink.
During a partial seizure the person does not usually fall down. The person may have sudden emotions or see, taste, or smell things that are not real. The person may seem to be in a dream. The muscles on one side of the body may jerk, or the person may repeat strange movements.
Causes
Many different things can cause epilepsy. It may result from a brain injury, either before or after birth, or a brain tumor. Diseases that affect the brain, including meningitis and encephalitis, can also lead to epilepsy. Epilepsy can sometimes occur after a person has a stroke (a blot clot or bleeding in the brain). Some cases of epilepsy may be genetic, or passed down from parent to child. In about half the cases of epilepsy the actual cause is not known.
Prevention
Because the cause of epilepsy is often unknown, the condition is difficult to prevent. People can prevent some types of epilepsy by protecting the brain from injury. Wearing a seat belt in cars can protect the head during an accident. Wearing a helmet while skating, biking, or playing sports can also prevent brain injury. Treating diseases and health problems that affect the brain can also help to prevent epilepsy.
Treatment
There is no cure for epilepsy, but there are a number of drugs that help to control seizures. A special diet can also help. If medicine and diet do not work, doctors may perform surgery on the brain. They may also place a small machine under the patient's skin. The machine sends electricity to the brain, which helps to reduce the number of seizures a person has.
People can help a person having a seizure by doing several things. They should help the person roll onto his side and put a pillow under his head. They should loosen the person's collar if possible. They should not put anything in the person's mouth. It is also important to move sharp or hard objects out of the person's way.
Monday, May 26, 2008
Microdermabrasion
Microdermabrasion is a mini procedure that involves the skin being "sandblasted" by aluminum oxide crystals, baking soda, salt or corn cob granules to remove the stratum corneum (top) layer of the skin; dead skin cells.
Microdermabrasion also promotes the production of new cells in the basal (deepest) layer of the dermis. This procedure may not give everyone the same results but if you have the money it is a nice treat and requires no down time. It can clean your pores incredibly and hinder any future breaks outs if used on a regular basis.
Are You Suitable for Microdermabrasion?
If you have or have had acne, discolorations, superficial lines and wrinkles, uneven texture or sun damaged skin -- you may be a candidate for Microdermabrasion.
Is Microdermabrasion Painful?
Microdermabrasion does not hurt although it may sting a little around the eye area. The patient normally works up to a level as they go to increase the penetration to the skin.
Microdermabrasion also promotes the production of new cells in the basal (deepest) layer of the dermis. This procedure may not give everyone the same results but if you have the money it is a nice treat and requires no down time. It can clean your pores incredibly and hinder any future breaks outs if used on a regular basis.
Are You Suitable for Microdermabrasion?
If you have or have had acne, discolorations, superficial lines and wrinkles, uneven texture or sun damaged skin -- you may be a candidate for Microdermabrasion.
Is Microdermabrasion Painful?
Microdermabrasion does not hurt although it may sting a little around the eye area. The patient normally works up to a level as they go to increase the penetration to the skin.
Medifast Diet: Complete Review
The Medifast diet plan is popular.
Forbes recently placed the company at number 28 in their 200 best small companies list), and Medifast have even produced a book (What Physicians Have Always Known About Weight Loss).
But what is Medifast all about? One clue is the name - it contains the word fast...
The Basics
The Medifast brand has been around for a number of decades, and at one time was only available via physicians. Nowadays the products can be ordered on-line and through a number of distributors.
Medifast offer a stable of meal replacement products - all generally formulated to be low-calorie and low-fat, and containing the optimum levels of vitamins. The formula will generally take users into a mild state of ketosis.
The most popular plan is called 5 and 1. This plan (800-1000 calories daily) comprises 5 meal replacements and one "real" meal containing a lean protein and vegetables and salad. Medifast claim a weight loss of 2-5 pounds per week on this plan.
Proof?
What many people don't realize is that very few commercial weight loss programs have ever undergone any clinical studies. Medifast heavily promote the fact that a Johns Hopkins university study has shown that Medifast results in significant weight loss (67 pound average loss in males and 57 pound average loss in females). It's worth pointing out that this study looked at patients who attended Medifast clinics.
There is also an additional study that compared the Medifast program with diabetes medication. The study found Medifast more effective at controlling type 2 diabetes than an ADA-recommended program (see PR).
Both studies were led by Associate Professor Lawrence Cheskin of Johns Hopkins Bloomberg School of Public Health and were funded by Medifast.
Successes
Due to the popularity of the program, Medifast have a number of "success stories" - one of which is Nnedi Uzowihe-Igwe of Maryland, USA (currently featured on the Medifast site). She also appeared in People magazine in January 2006 describing a massive transformation that resulted in a 160lb weight loss between June 2004 and April 2005. Nnedi subsequently became pregnant and gave birth to her second daughter)
I was able to find out how Nnedi was going now, and she appears to have maintained her massive initial weight loss (and is aiming to lose the weight she put on with the second baby by the end of this year).
What you can expect
Drastic
Protein fasts and low-calorie meal replacements are a drastic solution, and in my opinion appropriate for drastic situations. Given the choice between gastric bypass surgery or Medifast, then Medifast must surely be a better answer.
The biggest test of a program such as Medifast is the long-term consequences - and in particular weaning off a program based around shakes and soups. The transition phase should be four to six weeks, and often starts off by introducing some oatmeal at breakfast, and some fruit for snacks. Also exercise must become a part of life (5 days a week). Exercise must be fairly low-key during the restrictive part of Medifast - but once transitioning - it becomes increasingly important.
Due to the level of energy intake and exercise levels - it is likely that some muscle loss will occur during the weight loss phase. Once again, the best course of action would be to gradually include strength training during the transition phase - and begin to build up muscle tone.
Costs
The Medifast 5 and 1 plan cost $275 for 4 weeks. However - that's the cost of the "5" - you will still need to buy your daily "lean and green" meal (lean protein plus salad/vegetables).
Men & Women
Different formulations are used for men and women. Some shakes are called Medifast 55 or Medifast 70. The latter has a higher soy protein content and is more suitable for men (or women who prefer higher protein).
Behavior Change Required
Behavioral changes are critical to the long-term success of Medifast. Unless these lifestyle changes are applied, then the weight could easily swing back on like a yo-yo. It's worth taking a look at the post 10 Questions To Ask Before Changing Your Diet.
Conclusion
I don't believe Medifast is for the person who wants to lose 20 pounds. This is a serious program for serious situations, and it may be advisable to follow the program while receiving regular support from a clinic, and even under medical advisement.
However ample proof exists that the program does work and can lead to significant weight loss provided the transition phase is followed correctly.
Forbes recently placed the company at number 28 in their 200 best small companies list), and Medifast have even produced a book (What Physicians Have Always Known About Weight Loss).
But what is Medifast all about? One clue is the name - it contains the word fast...
The Basics
The Medifast brand has been around for a number of decades, and at one time was only available via physicians. Nowadays the products can be ordered on-line and through a number of distributors.
Medifast offer a stable of meal replacement products - all generally formulated to be low-calorie and low-fat, and containing the optimum levels of vitamins. The formula will generally take users into a mild state of ketosis.
The most popular plan is called 5 and 1. This plan (800-1000 calories daily) comprises 5 meal replacements and one "real" meal containing a lean protein and vegetables and salad. Medifast claim a weight loss of 2-5 pounds per week on this plan.
Proof?
What many people don't realize is that very few commercial weight loss programs have ever undergone any clinical studies. Medifast heavily promote the fact that a Johns Hopkins university study has shown that Medifast results in significant weight loss (67 pound average loss in males and 57 pound average loss in females). It's worth pointing out that this study looked at patients who attended Medifast clinics.
There is also an additional study that compared the Medifast program with diabetes medication. The study found Medifast more effective at controlling type 2 diabetes than an ADA-recommended program (see PR).
Both studies were led by Associate Professor Lawrence Cheskin of Johns Hopkins Bloomberg School of Public Health and were funded by Medifast.
Successes
Due to the popularity of the program, Medifast have a number of "success stories" - one of which is Nnedi Uzowihe-Igwe of Maryland, USA (currently featured on the Medifast site). She also appeared in People magazine in January 2006 describing a massive transformation that resulted in a 160lb weight loss between June 2004 and April 2005. Nnedi subsequently became pregnant and gave birth to her second daughter)
I was able to find out how Nnedi was going now, and she appears to have maintained her massive initial weight loss (and is aiming to lose the weight she put on with the second baby by the end of this year).
What you can expect
Drastic
Protein fasts and low-calorie meal replacements are a drastic solution, and in my opinion appropriate for drastic situations. Given the choice between gastric bypass surgery or Medifast, then Medifast must surely be a better answer.
The biggest test of a program such as Medifast is the long-term consequences - and in particular weaning off a program based around shakes and soups. The transition phase should be four to six weeks, and often starts off by introducing some oatmeal at breakfast, and some fruit for snacks. Also exercise must become a part of life (5 days a week). Exercise must be fairly low-key during the restrictive part of Medifast - but once transitioning - it becomes increasingly important.
Due to the level of energy intake and exercise levels - it is likely that some muscle loss will occur during the weight loss phase. Once again, the best course of action would be to gradually include strength training during the transition phase - and begin to build up muscle tone.
Costs
The Medifast 5 and 1 plan cost $275 for 4 weeks. However - that's the cost of the "5" - you will still need to buy your daily "lean and green" meal (lean protein plus salad/vegetables).
Men & Women
Different formulations are used for men and women. Some shakes are called Medifast 55 or Medifast 70. The latter has a higher soy protein content and is more suitable for men (or women who prefer higher protein).
Behavior Change Required
Behavioral changes are critical to the long-term success of Medifast. Unless these lifestyle changes are applied, then the weight could easily swing back on like a yo-yo. It's worth taking a look at the post 10 Questions To Ask Before Changing Your Diet.
Conclusion
I don't believe Medifast is for the person who wants to lose 20 pounds. This is a serious program for serious situations, and it may be advisable to follow the program while receiving regular support from a clinic, and even under medical advisement.
However ample proof exists that the program does work and can lead to significant weight loss provided the transition phase is followed correctly.
The Best Acne Treatments
There are too many acne fighting products on the market to count, and the majority of them simply do not work. However, there are some that do work quite well. The problem is that many people who suffer from acne will spend quite a bit of time and money trying to find the best acne treatments. Teenagers often outgrow acne before they find a treatment that works.
One of the better acne treatments on the market today is ProActiv. ProActiv seems to be helping many people who could not find other solutions that worked. It has been featured on infomercials, news stories, magazine articles, and newspaper articles. Proactiv is a system that includes a renewing cleanser, revitalizing toner, and repairing lotion. Prescription grade benzoyl peroxide is the active ingredient in ProActiv. ProActiv does not require a prescription.
A treatment that is available by prescription is Accutane. Accutane is a very strong medication, that is only suitable for those who suffer from severe and persistent acne. The medication is taken internally, and there are possible side effects, including birth defects, dry and cracked lips, and liver dysfunction.
Another one of that is used topically is retin-a. Many people have had great success with retin-a, which is used to treat acne, acne scars, wrinkles, stretch marks, skin discoloration, and a variety of other skin afflictions. Retin-a is available by prescription, but some over the counter medications contain retin-a.
Not all treatments come in the form of chemicals. Certain essential oils are also beneficial in the treatment of acne. These essential oils can be applied topically for the treatment of mild to moderate acne. The best essential oils for acne treatment are: Tea Tree Oil, Bergamot Oil, Clove Oil, Lavender Oil, and Rosewood Oil. If the essential oil needs to be diluted, mix it with Grapeseed Oil for best results.
In order to find the best acne treatment for you, start with essential oils. If that doesn't work, go to the next step by trying ProActive. If ProActive doesn't work, then try a prescription alternative. You may also consider being tested for food allergies, as certain allergies can cause acne. In this case, the only treatment you need is to eliminate those certain foods from your diet.
One of the better acne treatments on the market today is ProActiv. ProActiv seems to be helping many people who could not find other solutions that worked. It has been featured on infomercials, news stories, magazine articles, and newspaper articles. Proactiv is a system that includes a renewing cleanser, revitalizing toner, and repairing lotion. Prescription grade benzoyl peroxide is the active ingredient in ProActiv. ProActiv does not require a prescription.
A treatment that is available by prescription is Accutane. Accutane is a very strong medication, that is only suitable for those who suffer from severe and persistent acne. The medication is taken internally, and there are possible side effects, including birth defects, dry and cracked lips, and liver dysfunction.
Another one of that is used topically is retin-a. Many people have had great success with retin-a, which is used to treat acne, acne scars, wrinkles, stretch marks, skin discoloration, and a variety of other skin afflictions. Retin-a is available by prescription, but some over the counter medications contain retin-a.
Not all treatments come in the form of chemicals. Certain essential oils are also beneficial in the treatment of acne. These essential oils can be applied topically for the treatment of mild to moderate acne. The best essential oils for acne treatment are: Tea Tree Oil, Bergamot Oil, Clove Oil, Lavender Oil, and Rosewood Oil. If the essential oil needs to be diluted, mix it with Grapeseed Oil for best results.
In order to find the best acne treatment for you, start with essential oils. If that doesn't work, go to the next step by trying ProActive. If ProActive doesn't work, then try a prescription alternative. You may also consider being tested for food allergies, as certain allergies can cause acne. In this case, the only treatment you need is to eliminate those certain foods from your diet.
Friday, May 23, 2008
Mesothelioma
Mesothelioma is a form of cancer that is almost always caused by previous exposure to asbestos.[1] In this disease, malignant cells develop in the mesothelium, a protective lining that covers most of the body's internal organs. Its most common site is the pleura (outer lining of the lungs and chest cavity), but it may also occur in the peritoneum (the lining of the abdominal cavity) or the pericardium (a sac that surrounds the heart).
Most people who develop mesothelioma have worked on jobs where they inhaled asbestos particles, or have been exposed to asbestos dust and fibre in other ways, such as by washing the clothes of a family member who worked with asbestos, or by home renovation using asbestos cement products. Unlike lung cancer, there is no association between mesothelioma and smoking.
Signs and symptoms
Symptoms of mesothelioma may not appear until 20 to 50 years after exposure to asbestos. Shortness of breath, cough, and pain in the chest due to an accumulation of fluid in the pleural space are often symptoms of pleural mesothelioma.
Symptoms of peritoneal mesothelioma include weight loss and cachexia, abdominal swelling and pain due to ascites (a buildup of fluid in the abdominal cavity). Other symptoms of peritoneal mesothelioma may include bowel obstruction, blood clotting abnormalities, anemia, and fever. If the cancer has spread beyond the mesothelium to other parts of the body, symptoms may include pain, trouble swallowing, or swelling of the neck or face.
These symptoms may be caused by mesothelioma or by other, less serious conditions.
Mesothelioma that affects the pleura can cause these signs and symptoms:
* chest wall pain
* pleural effusion, or fluid surrounding the lung
* shortness of breath
* fatigue or anemia
* wheezing, hoarseness, or cough
* blood in the sputum (fluid) coughed up
In severe cases, the person may have many tumor masses. The individual may develop a pneumothorax, or collapse of the lung. The disease may metastasize, or spread, to other parts of the body.
Tumors that affect the abdominal cavity often do not cause symptoms until they are at a late stage. Symptoms include:
* abdominal pain
* ascites, or an abnormal buildup of fluid in the abdomen
* a mass in the abdomen
* problems with bowel function
* weight loss
In severe cases of the disease, the following signs and symptoms may be present:
* blood clots in the veins, which may cause thrombophlebitis
* disseminated intravascular coagulation, a disorder causing severe bleeding in many body organs
* jaundice, or yellowing of the eyes and skin
* low blood sugar level
* pleural effusion
* pulmonary emboli, or blood clots in the arteries of the lungs
* severe ascites
A mesothelioma does not usually spread to the bone, brain, or adrenal glands. Pleural tumors are usually found only on one side of the lungs.
Diagnosis
Diagnosing mesothelioma is often difficult, because the symptoms are similar to those of a number of other conditions. Diagnosis begins with a review of the patient's medical history. A history of exposure to asbestos may increase clinical suspicion for mesothelioma. A physical examination is performed, followed by chest X-ray and often lung function tests. The X-ray may reveal pleural thickening commonly seen after asbestos exposure and increases suspicion of mesothelioma. A CT (or CAT) scan or an MRI is usually performed. If a large amount of fluid is present, abnormal cells may be detected by cytology if this fluid is aspirated with a syringe. For pleural fluid this is done by a pleural tap or chest drain, in ascites with an paracentesis or ascitic drain and in a pericardial effusion with pericardiocentesis. While absence of malignant cells on cytology does not completely exclude mesothelioma, it makes it much more unlikely, especially if an alternative diagnosis can be made (e.g. tuberculosis, heart failure).
If cytology is positive or a plaque is regarded as suspicious, a biopsy is needed to confirm a diagnosis of mesothelioma. A doctor removes a sample of tissue for examination under a microscope by a pathologist. A biopsy may be done in different ways, depending on where the abnormal area is located. If the cancer is in the chest, the doctor may perform a thoracoscopy. In this procedure, the doctor makes a small cut through the chest wall and puts a thin, lighted tube called a thoracoscope into the chest between two ribs. Thoracoscopy allows the doctor to look inside the chest and obtain tissue samples.
If the cancer is in the abdomen, the doctor may perform a laparoscopy. To obtain tissue for examination, the doctor makes a small opening in the abdomen and inserts a special instrument into the abdominal cavity. If these procedures do not yield enough tissue, more extensive diagnostic surgery may be necessary.
Doctors have begun testing the Mesomark assay which measures levels of soluble mesothelin-related proteins (SMRPs) released by diseased mesothelioma cells. The procedure could diagnose mesothelioma earlier than conventional methods thus improving the survival prospects for patients
Treatment
Treatment of MM using conventional therapies has not proved successful and patients have a median survival time of 6 - 12 months after presentation[citation needed]. The clinical behaviour of the malignancy is affected by several factors including the continuous mesothelial surface of the pleural cavity which favours local metastasis via exfoliated cells, invasion to underlying tissue and other organs within the pleural cavity, and the extremely long latency period between asbestos exposure and development of the disease.
Surgery
Surgery, either by itself or used in combination with pre- and post-operative adjuvant therapies, has proved disappointing. A pleurectomy/decortication is the most common surgery, in which the lining of the chest is removed. Less common is an extrapleural pneumonectomy (EPP), in which the lung, lining of the inside of the chest, the hemi-diaphragm and the pericardium are removed. It is not possible to remove the entire mesothelium without killing the patient.
Radiation
For patients with localized disease, and who can tolerate a radical surgery, radiation is often given post-operatively as a consolidative treatment. The entire hemi-thorax is treated with radiation therapy, often given simultaneously with chemotherapy. This approach of using surgery followed by radiation with chemotherapy has been pioneered by the thoracic oncology team at Brigham & Women's Hospital in Boston.Delivering radiation and chemotherapy after a radical surgery has led to extended life expectancy in selected patient populations with some patients surviving more than 5 years. As part of a curative approach to mesothelioma, radiotherapy is also commonly applied to the sites of chest drain insertion, in order to prevent growth of the tumor along the track in the chest wall.
Although mesothelioma is generally resistant to curative treatment with radiotherapy alone, palliative treatment regimens are sometimes used to relieve symptoms arising from tumor growth, such as obstruction of a major blood vessel. Radiation therapy when given alone with curative intent has never been shown to improve survival from mesothelioma. The necessary radiation dose to treat mesothelioma that has not been surgically removed would be very toxic.
Chemotherapy
In February 2004, the United States Food and Drug Administration approved pemetrexed (brand name Alimta) for treatment of malignant pleural mesothelioma. Pemetrexed is given in combination with cisplatin. Folic acid is also used to reduce the side-effects of pemetrexed.
Immunotherapy
Treatment regimens involving immunotherapy have yielded variable results. For example, intrapleural inoculation of Bacillus Calmette-Guérin (BCG) in an attempt to boost the immune response, was found to be of no benefit to the patient (while it may benefit patients with bladder cancer). Mesothelioma cells proved susceptible to in vitro lysis by LAK cells following activation by interleukin-2 (IL-2), but patients undergoing this particular therapy experienced major side effects. Indeed, this trial was suspended in view of the unacceptably high levels of IL-2 toxicity and the severity of side effects such as fever and cachexia. Nonetheless, other trials involving interferon alpha have proved more encouraging with 20% of patients experiencing a greater than 50% reduction in tumor mass combined with minimal side effects.
Heated Intraoperative Intraperitoneal Chemotherapy
A procedure known as heated intraoperative intraperitoneal chemotherapy was developed by Paul Sugarbaker at the Washington Cancer Institute.The surgeon removes as much of the tumor as possible followed by the direct administration of a chemotherapy agent, heated to between 40 and 48°C, in the abdomen. The fluid is perfused for 60 to 120 minutes and then drained.
This technique permits the administration of high concentrations of selected drugs into the abdominal and pelvic surfaces. Heating the chemotherapy treatment increases the penetration of the drugs into tissues. Also, heating itself damages the malignant cells more than the normal cells.
Most people who develop mesothelioma have worked on jobs where they inhaled asbestos particles, or have been exposed to asbestos dust and fibre in other ways, such as by washing the clothes of a family member who worked with asbestos, or by home renovation using asbestos cement products. Unlike lung cancer, there is no association between mesothelioma and smoking.
Signs and symptoms
Symptoms of mesothelioma may not appear until 20 to 50 years after exposure to asbestos. Shortness of breath, cough, and pain in the chest due to an accumulation of fluid in the pleural space are often symptoms of pleural mesothelioma.
Symptoms of peritoneal mesothelioma include weight loss and cachexia, abdominal swelling and pain due to ascites (a buildup of fluid in the abdominal cavity). Other symptoms of peritoneal mesothelioma may include bowel obstruction, blood clotting abnormalities, anemia, and fever. If the cancer has spread beyond the mesothelium to other parts of the body, symptoms may include pain, trouble swallowing, or swelling of the neck or face.
These symptoms may be caused by mesothelioma or by other, less serious conditions.
Mesothelioma that affects the pleura can cause these signs and symptoms:
* chest wall pain
* pleural effusion, or fluid surrounding the lung
* shortness of breath
* fatigue or anemia
* wheezing, hoarseness, or cough
* blood in the sputum (fluid) coughed up
In severe cases, the person may have many tumor masses. The individual may develop a pneumothorax, or collapse of the lung. The disease may metastasize, or spread, to other parts of the body.
Tumors that affect the abdominal cavity often do not cause symptoms until they are at a late stage. Symptoms include:
* abdominal pain
* ascites, or an abnormal buildup of fluid in the abdomen
* a mass in the abdomen
* problems with bowel function
* weight loss
In severe cases of the disease, the following signs and symptoms may be present:
* blood clots in the veins, which may cause thrombophlebitis
* disseminated intravascular coagulation, a disorder causing severe bleeding in many body organs
* jaundice, or yellowing of the eyes and skin
* low blood sugar level
* pleural effusion
* pulmonary emboli, or blood clots in the arteries of the lungs
* severe ascites
A mesothelioma does not usually spread to the bone, brain, or adrenal glands. Pleural tumors are usually found only on one side of the lungs.
Diagnosis
Diagnosing mesothelioma is often difficult, because the symptoms are similar to those of a number of other conditions. Diagnosis begins with a review of the patient's medical history. A history of exposure to asbestos may increase clinical suspicion for mesothelioma. A physical examination is performed, followed by chest X-ray and often lung function tests. The X-ray may reveal pleural thickening commonly seen after asbestos exposure and increases suspicion of mesothelioma. A CT (or CAT) scan or an MRI is usually performed. If a large amount of fluid is present, abnormal cells may be detected by cytology if this fluid is aspirated with a syringe. For pleural fluid this is done by a pleural tap or chest drain, in ascites with an paracentesis or ascitic drain and in a pericardial effusion with pericardiocentesis. While absence of malignant cells on cytology does not completely exclude mesothelioma, it makes it much more unlikely, especially if an alternative diagnosis can be made (e.g. tuberculosis, heart failure).
If cytology is positive or a plaque is regarded as suspicious, a biopsy is needed to confirm a diagnosis of mesothelioma. A doctor removes a sample of tissue for examination under a microscope by a pathologist. A biopsy may be done in different ways, depending on where the abnormal area is located. If the cancer is in the chest, the doctor may perform a thoracoscopy. In this procedure, the doctor makes a small cut through the chest wall and puts a thin, lighted tube called a thoracoscope into the chest between two ribs. Thoracoscopy allows the doctor to look inside the chest and obtain tissue samples.
If the cancer is in the abdomen, the doctor may perform a laparoscopy. To obtain tissue for examination, the doctor makes a small opening in the abdomen and inserts a special instrument into the abdominal cavity. If these procedures do not yield enough tissue, more extensive diagnostic surgery may be necessary.
Doctors have begun testing the Mesomark assay which measures levels of soluble mesothelin-related proteins (SMRPs) released by diseased mesothelioma cells. The procedure could diagnose mesothelioma earlier than conventional methods thus improving the survival prospects for patients
Treatment
Treatment of MM using conventional therapies has not proved successful and patients have a median survival time of 6 - 12 months after presentation[citation needed]. The clinical behaviour of the malignancy is affected by several factors including the continuous mesothelial surface of the pleural cavity which favours local metastasis via exfoliated cells, invasion to underlying tissue and other organs within the pleural cavity, and the extremely long latency period between asbestos exposure and development of the disease.
Surgery
Surgery, either by itself or used in combination with pre- and post-operative adjuvant therapies, has proved disappointing. A pleurectomy/decortication is the most common surgery, in which the lining of the chest is removed. Less common is an extrapleural pneumonectomy (EPP), in which the lung, lining of the inside of the chest, the hemi-diaphragm and the pericardium are removed. It is not possible to remove the entire mesothelium without killing the patient.
Radiation
For patients with localized disease, and who can tolerate a radical surgery, radiation is often given post-operatively as a consolidative treatment. The entire hemi-thorax is treated with radiation therapy, often given simultaneously with chemotherapy. This approach of using surgery followed by radiation with chemotherapy has been pioneered by the thoracic oncology team at Brigham & Women's Hospital in Boston.Delivering radiation and chemotherapy after a radical surgery has led to extended life expectancy in selected patient populations with some patients surviving more than 5 years. As part of a curative approach to mesothelioma, radiotherapy is also commonly applied to the sites of chest drain insertion, in order to prevent growth of the tumor along the track in the chest wall.
Although mesothelioma is generally resistant to curative treatment with radiotherapy alone, palliative treatment regimens are sometimes used to relieve symptoms arising from tumor growth, such as obstruction of a major blood vessel. Radiation therapy when given alone with curative intent has never been shown to improve survival from mesothelioma. The necessary radiation dose to treat mesothelioma that has not been surgically removed would be very toxic.
Chemotherapy
In February 2004, the United States Food and Drug Administration approved pemetrexed (brand name Alimta) for treatment of malignant pleural mesothelioma. Pemetrexed is given in combination with cisplatin. Folic acid is also used to reduce the side-effects of pemetrexed.
Immunotherapy
Treatment regimens involving immunotherapy have yielded variable results. For example, intrapleural inoculation of Bacillus Calmette-Guérin (BCG) in an attempt to boost the immune response, was found to be of no benefit to the patient (while it may benefit patients with bladder cancer). Mesothelioma cells proved susceptible to in vitro lysis by LAK cells following activation by interleukin-2 (IL-2), but patients undergoing this particular therapy experienced major side effects. Indeed, this trial was suspended in view of the unacceptably high levels of IL-2 toxicity and the severity of side effects such as fever and cachexia. Nonetheless, other trials involving interferon alpha have proved more encouraging with 20% of patients experiencing a greater than 50% reduction in tumor mass combined with minimal side effects.
Heated Intraoperative Intraperitoneal Chemotherapy
A procedure known as heated intraoperative intraperitoneal chemotherapy was developed by Paul Sugarbaker at the Washington Cancer Institute.The surgeon removes as much of the tumor as possible followed by the direct administration of a chemotherapy agent, heated to between 40 and 48°C, in the abdomen. The fluid is perfused for 60 to 120 minutes and then drained.
This technique permits the administration of high concentrations of selected drugs into the abdominal and pelvic surfaces. Heating the chemotherapy treatment increases the penetration of the drugs into tissues. Also, heating itself damages the malignant cells more than the normal cells.
Alzheimer disease
degenerative brain disorder that develops in mid to late adulthood. It results in a progressive and irreversible decline in memory and a deterioration of various other cognitive abilities. The disease is characterized by the destruction of nerve cells and neural connections in the cerebral cortex of the brain and by a significant loss of brain mass. The disease was first described in 1906 by Alois Alzheimer, a German neuropathologist.
Alzheimer disease is the most common form of *dementia. The disease develops differently among individuals; this suggests that more than one pathologic process may lead to the same outcome. Typically, the first symptom to appear is forgetfulness. As the disease progresses, memory loss becomes more severe, and language, perceptual, and motor skills deteriorate. Mood becomes unstable, and the individual tends to become irritable and more sensitive to stress and may become intermittently angry, anxious, or depressed. In advanced stages, the individual becomes unresponsive and loses mobility and control of body functions; death ensues after a disease course lasting from 2 to 20 years.
About 10 percent of those who develop the disease are younger than 60 years of age. These cases, referred to as early-onset familial Alzheimer disease, result from an inherited genetic mutation. The majority of cases of Alzheimer disease, however, develop after age 60 (late-onset); they usually occur sporadically—i.e., in individuals with no family history of the disease—although a genetic factor has been identified that is thought to predispose these individuals to the disorder.
The presence of neuritic plaques and neurofibrillary tangles in the brain are used to diagnose Alzheimer disease in autopsy. Neuritic plaques—also called senile, dendritic, or amyloid plaques—consist of deteriorating neuronal material surrounding deposits of a sticky protein called beta amyloid. This protein is derived from a larger molecule called amyloid precursor protein, which is a normal component of nerve cells. Neurofibrillary tangles are twisted protein fibres located within nerve cells. These fibres consist of a protein, called tau, that normally occurs in neurons. When incorrectly processed, tau molecules clump together and form tangles. Both neuritic plaques and neurofibrillary tangles, which also may be found in smaller amounts in the brains of healthy elderly persons, are thought to interfere in some way with normal cellular functioning. However, it is not known whether the plaques and tangles are a cause or a consequence of the disease.
Other features have been noted in the brains of many persons with Alzheimer disease. One is a deficiency of the neurotransmitter acetylcholine; neurons containing acetylcholine play an important role in memory. Abnormal concentrations of aluminum also have been found in neurofibrillary tangles and neuritic plaques, but it is not known whether the element plays a causative role in the disease.
Underlying genetic defects have been identified for both late- and early-onset cases of Alzheimer disease. A defect in the gene that codes for amyloid precursor protein may increase the production or deposition of beta amyloid, which forms the core of neuritic plaques. This gene, however, is responsible for only 2 to 3 percent of all early-onset cases of the disease; the remainder are attributed to two other genes. A defect in the gene that directs production of apolipoprotein E (ApoE), which is involved in cholesterol transport, may be a factor in the majority of late-onset Alzheimer cases. There are three forms of this gene—ApoE2, ApoE3, and ApoE4—one of which, ApoE4, is associated with a higher risk of disease.
There is no cure for Alzheimer disease. The medication tacrine slightly slows the progression of the disease by slowing the breakdown of acetylcholine, but it is not effective in all patients and can become toxic to the liver. Most treatment aims to control the depression, behavioral problems, and insomnia that often accompany the disease.
*dementia
chronic, usually progressive deterioration of intellectual capacity associated with the widespread loss of nerve cells and the shrinkage of brain tissue. Dementia is most commonly seen in the elderly (senile dementia), though it is not part of the normal aging process and can affect persons of any age.
The most common irreversible dementia is Alzheimer disease. This condition begins with memory loss, which may first appear to be simple absentmindedness or forgetfulness. As dementia progresses, the loss of memory broadens in scope until the individual can no longer remember basic social and survival skills or function independently. Language, spatial or temporal orientation, judgment, or other cognitive capacities may decline, and personality changes may also occur. Dementia is also present in other degenerative brain diseases including Pick disease and Parkinson disease.
The second most common cause of dementia is hypertension (high blood pressure) or other vascular conditions. This type of dementia, called multi-infarct, or vascular, dementia results from a series of small strokes that progressively destroy the brain. Dementia can also be caused by Huntington disease, syphilis, multiple sclerosis, acquired immune deficiency syndrome (AIDS), and some types of encephalitis. Treatable dementias occur in hypothyroidism, other metabolic diseases, and some malignant tumours. Treatment of the underlying disease in these cases may inhibit the progress of dementia but usually does not reverse it.
Alzheimer disease is the most common form of *dementia. The disease develops differently among individuals; this suggests that more than one pathologic process may lead to the same outcome. Typically, the first symptom to appear is forgetfulness. As the disease progresses, memory loss becomes more severe, and language, perceptual, and motor skills deteriorate. Mood becomes unstable, and the individual tends to become irritable and more sensitive to stress and may become intermittently angry, anxious, or depressed. In advanced stages, the individual becomes unresponsive and loses mobility and control of body functions; death ensues after a disease course lasting from 2 to 20 years.
About 10 percent of those who develop the disease are younger than 60 years of age. These cases, referred to as early-onset familial Alzheimer disease, result from an inherited genetic mutation. The majority of cases of Alzheimer disease, however, develop after age 60 (late-onset); they usually occur sporadically—i.e., in individuals with no family history of the disease—although a genetic factor has been identified that is thought to predispose these individuals to the disorder.
The presence of neuritic plaques and neurofibrillary tangles in the brain are used to diagnose Alzheimer disease in autopsy. Neuritic plaques—also called senile, dendritic, or amyloid plaques—consist of deteriorating neuronal material surrounding deposits of a sticky protein called beta amyloid. This protein is derived from a larger molecule called amyloid precursor protein, which is a normal component of nerve cells. Neurofibrillary tangles are twisted protein fibres located within nerve cells. These fibres consist of a protein, called tau, that normally occurs in neurons. When incorrectly processed, tau molecules clump together and form tangles. Both neuritic plaques and neurofibrillary tangles, which also may be found in smaller amounts in the brains of healthy elderly persons, are thought to interfere in some way with normal cellular functioning. However, it is not known whether the plaques and tangles are a cause or a consequence of the disease.
Other features have been noted in the brains of many persons with Alzheimer disease. One is a deficiency of the neurotransmitter acetylcholine; neurons containing acetylcholine play an important role in memory. Abnormal concentrations of aluminum also have been found in neurofibrillary tangles and neuritic plaques, but it is not known whether the element plays a causative role in the disease.
Underlying genetic defects have been identified for both late- and early-onset cases of Alzheimer disease. A defect in the gene that codes for amyloid precursor protein may increase the production or deposition of beta amyloid, which forms the core of neuritic plaques. This gene, however, is responsible for only 2 to 3 percent of all early-onset cases of the disease; the remainder are attributed to two other genes. A defect in the gene that directs production of apolipoprotein E (ApoE), which is involved in cholesterol transport, may be a factor in the majority of late-onset Alzheimer cases. There are three forms of this gene—ApoE2, ApoE3, and ApoE4—one of which, ApoE4, is associated with a higher risk of disease.
There is no cure for Alzheimer disease. The medication tacrine slightly slows the progression of the disease by slowing the breakdown of acetylcholine, but it is not effective in all patients and can become toxic to the liver. Most treatment aims to control the depression, behavioral problems, and insomnia that often accompany the disease.
*dementia
chronic, usually progressive deterioration of intellectual capacity associated with the widespread loss of nerve cells and the shrinkage of brain tissue. Dementia is most commonly seen in the elderly (senile dementia), though it is not part of the normal aging process and can affect persons of any age.
The most common irreversible dementia is Alzheimer disease. This condition begins with memory loss, which may first appear to be simple absentmindedness or forgetfulness. As dementia progresses, the loss of memory broadens in scope until the individual can no longer remember basic social and survival skills or function independently. Language, spatial or temporal orientation, judgment, or other cognitive capacities may decline, and personality changes may also occur. Dementia is also present in other degenerative brain diseases including Pick disease and Parkinson disease.
The second most common cause of dementia is hypertension (high blood pressure) or other vascular conditions. This type of dementia, called multi-infarct, or vascular, dementia results from a series of small strokes that progressively destroy the brain. Dementia can also be caused by Huntington disease, syphilis, multiple sclerosis, acquired immune deficiency syndrome (AIDS), and some types of encephalitis. Treatable dementias occur in hypothyroidism, other metabolic diseases, and some malignant tumours. Treatment of the underlying disease in these cases may inhibit the progress of dementia but usually does not reverse it.
Hodgkin disease
an uncommon cancer of the lymphatic system (malignant lymphoma) that usually strikes young adults and people 55 years of age or older. Most patients can be cured if the disease is detected in its early stages, but even those with advanced Hodgkin disease have a significant chance of recovery. The overall cure rate is approximately 75 percent.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
Pick disease
form of premature dementia caused by atrophy of the frontal and temporal lobes of the brain. It resembles Alzheimer disease but is much less common. Pick disease is characterized by a progressive deterioration of intellect, judgment, and memory, resulting in increased irritability, inappropriate behaviour, depression, and paranoia. Histologically some cerebral nerve cells are swollen and contain abnormal inclusions called Pick bodies. The cause of Pick disease is unknown, but in some cases the disease appears to be inherited. Average survival from onset (generally between the ages of 40 and 60) to death is about 10 years; there is no specific treatment. The disease was first described by the German neurologist Arnold Pick.
Plummer's disease
also called toxic multinodular goitre thyroid condition characterized by marked enlargement of the thyroid gland (goitre), firm thyroid nodules, and mild overproduction of thyroid hormone (hyperthyroidism). Plummer's disease, which usually occurs in older people, is of unknown etiology. Its symptoms resemble those of Graves' disease (q.v.), a condition believed to be an autoimmune disorder caused by antibodies to the thyroid.
Typically, persons affected by Plummer's disease develop a goitre many years before the onset of symptoms of hyperthyroidism; most patients are over age 50 before the characteristic accelerated heart rate and other cardiac conditions appear. Unlike other forms of hyperthyroidism, the disease seldom causes bulging of the eyes (exophthalmos). Swelling of the thyroid gland may obstruct breathing or swallowing, requiring surgery to remove the excess tissue; the cardiac symptoms, resulting in congestive heart failure in some cases, can also be fatal. In the absence of obstruction or cosmetic reasons for removing the gland, the goitre may be treated with drugs that block thyroid activity or with radioactive iodine therapy; however, the multiple thyroid nodules characteristic of the disease may raise suspicion of cancer, necessitating surgical excision of the gland.
Typically, persons affected by Plummer's disease develop a goitre many years before the onset of symptoms of hyperthyroidism; most patients are over age 50 before the characteristic accelerated heart rate and other cardiac conditions appear. Unlike other forms of hyperthyroidism, the disease seldom causes bulging of the eyes (exophthalmos). Swelling of the thyroid gland may obstruct breathing or swallowing, requiring surgery to remove the excess tissue; the cardiac symptoms, resulting in congestive heart failure in some cases, can also be fatal. In the absence of obstruction or cosmetic reasons for removing the gland, the goitre may be treated with drugs that block thyroid activity or with radioactive iodine therapy; however, the multiple thyroid nodules characteristic of the disease may raise suspicion of cancer, necessitating surgical excision of the gland.
Huntington disease
also called Huntington chorea a relatively rare, and invariably fatal, hereditary neurological disease that is characterized by irregular and involuntary movements of the muscles. Huntington disease is caused by a genetic mutation that causes degeneration of neurons in the basal ganglia, a pair of nerve clusters deep within the brain, that control movement. Symptoms usually appear between the ages of 35 and 50 and worsen over time. They begin with occasional jerking or writhing movements, called choreiform movements, or what appear to be minor problems with coordination; these movements, which are absent during sleep, worsen over the next few years and progress to random, uncontrollable, and often violent twitchings and jerks. Symptoms of mental deterioration may appear including apathy, fatigue, irritability, restlessness, or moodiness; these symptoms may progress to memory loss, dementia, bipolar disorder, or schizophrenia. The disease was first described by the American physician George Huntington in 1872.
Simmonds' disease
pituitary disorder characterized by panhypopituitarism, a form of hypopituitarism in which all pituitary secretions are deficient. Effects include dwarfism, atrophy of the sex glands, shrinkage of the breasts and suppression of milk secretion, atrophy of the thyroid and the adrenal cortex, lowering of the metabolic rate, tendency toward lowered blood sugar, and lessened resistance to infection and shock. Some effects of panhypopituitarism have been simulated among emotionally deprived young children. Such children have shown remarkable recovery when removed from the injurious environment. The German doctor Morris Simmonds (1855–1925) first described this disease in 1914.
McArdle's disease
also called Glycogenosis Type V, rare hereditary deficiency of the enzyme glycogen phosphorylase in muscle cells. In the absence of this enzyme, muscles cannot break down animal starch (glycogen) to meet the energy requirements of exercise. Muscle activity is thus solely dependent on the availability of glucose (blood sugar) and other nutrients in the circulating blood. Victims of McArdle's disease are chronically weak because their muscles are incapable of prolonged exertion; even moderate exercise produces muscle cramping and severe pain. Unlike most other types of glycogenosis, the disease is not fatal, and the missing enzyme does not impair the functioning of other body systems. McArdle's disease is inherited as an autosomal recessive trait
Rabies
also called hydrophobia , or lyssa acute, usually fatal, viral infectious disease of the central nervous system. The disease is usually spread among domestic dogs and wild carnivorous animals; all warm-blooded animals are susceptible to rabies infection. The virus, a rhabdovirus, is often present in the salivary glands of rabid animals and is excreted in the saliva; thus, the bite of the infected animal introduces the virus into a fresh wound. Under favourable conditions, the virus propagates along nerve tissue from the wound to the brain and becomes established in the central nervous system. The disease develops most often between four and six weeks after infection, but the incubation period may vary from 10 days to eight months.
Rabies often begins with excitation of the central nervous system expressed as irritability and viciousness. A rabid animal is most dangerous during the early stages of the disease because it appears to be healthy and may seem friendly but will bite at the slightest provocation. Wild animals that appear to be tame and that approach people or human habitations in the daytime should be suspected of having rabies.
Infected dogs usually show a short excitation phase that is characterized by restlessness, nervousness, irritability, and viciousness and is followed by depression and paralysis. Sudden death without recognizable signs of illness is common. Dogs that develop the predominantly excited type of rabies invariably die of the infection, usually within three to five days after the onset of symptoms. Those that develop the paralytic type of rabies without any evidence of excitation or viciousness may recover on rare occasions. Paralysis of the “voice” muscles in rabid dogs may produce a characteristic change in the sound of the bark.
Rabies in humans is similar to that in animals. Symptoms include depression, headache, nausea, seizures, anorexia, muscle stiffness, and increased production of saliva. Abnormal sensations, such as itching, around the site of exposure are a common early symptom. Repeated episodes of painful contraction of the muscles of the throat may occur upon attempting to swallow or may be elicited by the sight of water. This reaction to water is called hydrophobia (“fear of water”). Rabies in humans is almost always fatal. Death ordinarily occurs within three to five days after the onset of symptoms due to cardiac or respiratory failure. Sometimes rabies is characterized by paralysis without any evidence of excitation of the nervous system. In such cases the course of the disease may be prolonged to a week or more.
If administered soon after infection, serum or vaccine can be effective in combating the disease. This is a type of passive immunization whereby animals are immunized with attenuated rabies virus, and antibodies from these animals are injected into infected persons to give them temporary immunity to rabies. The treatment is effective if given within 24 hours after exposure but has little, if any, value if given three or more days after infection by rabies. Immediate treatment of animal-bite wounds by cleansing with soap and water is extremely important because much, if not all, of the virus can be thus removed.
Vaccines prepared from rabies virus can be used to protect people who are likely to be in contact with infected animals. The safest and most effective vaccines are human diploidcell vaccine (HDCV), purified chick embryo cell culture (PCEC), and rabies vaccine adsorbed (RVA). When a person not protected by previous immunization is bitten by a rabid animal, treatment is a dose of serum followed by a series of vaccinations. With the older vaccines, at least 16 injections were required, whereas with HDCV, PCEC, or RVA, 5 are usually sufficient.
Rabies often begins with excitation of the central nervous system expressed as irritability and viciousness. A rabid animal is most dangerous during the early stages of the disease because it appears to be healthy and may seem friendly but will bite at the slightest provocation. Wild animals that appear to be tame and that approach people or human habitations in the daytime should be suspected of having rabies.
Infected dogs usually show a short excitation phase that is characterized by restlessness, nervousness, irritability, and viciousness and is followed by depression and paralysis. Sudden death without recognizable signs of illness is common. Dogs that develop the predominantly excited type of rabies invariably die of the infection, usually within three to five days after the onset of symptoms. Those that develop the paralytic type of rabies without any evidence of excitation or viciousness may recover on rare occasions. Paralysis of the “voice” muscles in rabid dogs may produce a characteristic change in the sound of the bark.
Rabies in humans is similar to that in animals. Symptoms include depression, headache, nausea, seizures, anorexia, muscle stiffness, and increased production of saliva. Abnormal sensations, such as itching, around the site of exposure are a common early symptom. Repeated episodes of painful contraction of the muscles of the throat may occur upon attempting to swallow or may be elicited by the sight of water. This reaction to water is called hydrophobia (“fear of water”). Rabies in humans is almost always fatal. Death ordinarily occurs within three to five days after the onset of symptoms due to cardiac or respiratory failure. Sometimes rabies is characterized by paralysis without any evidence of excitation of the nervous system. In such cases the course of the disease may be prolonged to a week or more.
If administered soon after infection, serum or vaccine can be effective in combating the disease. This is a type of passive immunization whereby animals are immunized with attenuated rabies virus, and antibodies from these animals are injected into infected persons to give them temporary immunity to rabies. The treatment is effective if given within 24 hours after exposure but has little, if any, value if given three or more days after infection by rabies. Immediate treatment of animal-bite wounds by cleansing with soap and water is extremely important because much, if not all, of the virus can be thus removed.
Vaccines prepared from rabies virus can be used to protect people who are likely to be in contact with infected animals. The safest and most effective vaccines are human diploidcell vaccine (HDCV), purified chick embryo cell culture (PCEC), and rabies vaccine adsorbed (RVA). When a person not protected by previous immunization is bitten by a rabid animal, treatment is a dose of serum followed by a series of vaccinations. With the older vaccines, at least 16 injections were required, whereas with HDCV, PCEC, or RVA, 5 are usually sufficient.
Pompe's disease
also called Glycogenosis Type Ii, hereditary defect in the body's ability to metabolize glycogen, resulting in a muscle disorder that is usually fatal during the first year of life. The defect responsible, absence of the enzyme alpha-1,4-glucosidase, is extremely rare, occurring in fewer than one in every 150,000 births, and is transmitted as an autosomal recessive trait. In Pompe's disease, glycogen accumulates in all body tissues, but especially in the muscles, causing enlargement of the heart, cardiac muscle failure, and breathing difficulties. Accumulation of glycogen in other tissues causes mental retardation and enlargement of the liver and spleen. Death usually results from cardiorespiratory failure. Juvenile and adult forms, with similar but milder symptoms, are also known.
Chicken pox
One of the most common diseases of childhood is chicken pox. This disease is caused by a virus. Although most patients contract it between the ages of 2 and 6, chicken pox can strike at any age. Chicken pox is a fairly mild illness in children. It can be very serious in adults, however. It is also extremely serious in people with certain diseases such as leukemia or AIDS because their immune systems are weak and therefore they cannot fight off the disease.
How chicken pox is spread
Chicken pox is highly contagious, meaning that it can spread very easily. When an infected person coughs or sneezes, tiny particles of the virus are released into the air. The disease can be spread when an uninfected person inhales these particles. The virus particles can also be on the clothing or bedding of an infected patient. If an uninfected person touches the clothing or bedding he or she can become infected with the disease.
Symptoms
The first symptoms, or signs of the disease, are very general and resemble those of the flu. These include a slight fever, runny nose, and mild cough. The patient will not feel very hungry and may also have headaches and feel very tired.
Roughly two weeks after being exposed to the virus, red spots appear on the face and body. These spots are filled with fluid, and they itch terribly. Eventually the spots form scabs, which soon fall off.
Treatment
People with chicken pox should try not to scratch the spots. Scratching can cause the spots to leave deep scars. The itching can be relieved by using medications such as calamine lotion, which has a soothing effect. In addition to using calamine lotion, patients may wish to bathe the pox spots and sores with cool water. It is important to keep the spots clean so that they do not become further infected with other harmful germs. Bed rest is important.
It is extremely important to never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany chicken pox. Using aspirin to treat chicken pox has been connected to the development of a severe disease called Reye syndrome. This syndrome can cause liver and brain damage, and even death.
A case of chicken pox generally lasts from a week to ten days overall. Because the disease is so contagious, it is important for the patient to remain confined to bed until the scabs have fallen off. Complications are rare but can occur in some cases. In some instances, the virus becomes dormant. This means that it remains in the body but no longer causes the symptoms of chicken pox. In these cases, it is possible for the virus to become re-activated in adulthood, when it causes a related disease called shingles. Scientists developed a chicken pox vaccine, or substance that protects people from getting the disease, in the late 20th century.
How chicken pox is spread
Chicken pox is highly contagious, meaning that it can spread very easily. When an infected person coughs or sneezes, tiny particles of the virus are released into the air. The disease can be spread when an uninfected person inhales these particles. The virus particles can also be on the clothing or bedding of an infected patient. If an uninfected person touches the clothing or bedding he or she can become infected with the disease.
Symptoms
The first symptoms, or signs of the disease, are very general and resemble those of the flu. These include a slight fever, runny nose, and mild cough. The patient will not feel very hungry and may also have headaches and feel very tired.
Roughly two weeks after being exposed to the virus, red spots appear on the face and body. These spots are filled with fluid, and they itch terribly. Eventually the spots form scabs, which soon fall off.
Treatment
People with chicken pox should try not to scratch the spots. Scratching can cause the spots to leave deep scars. The itching can be relieved by using medications such as calamine lotion, which has a soothing effect. In addition to using calamine lotion, patients may wish to bathe the pox spots and sores with cool water. It is important to keep the spots clean so that they do not become further infected with other harmful germs. Bed rest is important.
It is extremely important to never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany chicken pox. Using aspirin to treat chicken pox has been connected to the development of a severe disease called Reye syndrome. This syndrome can cause liver and brain damage, and even death.
A case of chicken pox generally lasts from a week to ten days overall. Because the disease is so contagious, it is important for the patient to remain confined to bed until the scabs have fallen off. Complications are rare but can occur in some cases. In some instances, the virus becomes dormant. This means that it remains in the body but no longer causes the symptoms of chicken pox. In these cases, it is possible for the virus to become re-activated in adulthood, when it causes a related disease called shingles. Scientists developed a chicken pox vaccine, or substance that protects people from getting the disease, in the late 20th century.
Mumps
One of the most common and highly contagious diseases of childhood is mumps. This disease is caused by a virus that infects a pair of glands located in front of the ears. When the glands are infected, they become swollen. This gives the cheeks a chipmunk-like appearance. Although mumps can infect adults, it is more commonly found in children between the ages of 5 and 15 years
How mumps is spread
The glands that are infected by the mumps virus normally produce saliva. Because of this, when a person is infected, pieces of the virus become mixed in with the saliva produced by the glands. Any contact with the saliva of an infected person can therefore spread the disease.When an infected person coughs or sneezes, tiny particles of the virus are spread into the air. If these are inhaled by an uninfected person or a person who has not been vaccinated against the disease, that person will become ill with mumps. The disease can also be spread by touching something, such as bedding, that has infected saliva on it.
Symptoms
Once a person is infected with the mumps virus, it usually takes two to three weeks for symptoms, or signs of the disease, to appear. The first symptoms a patient will feel are very general and resemble those of the flu. The patient may have a runny nose and a slight fever. Soon the area in front of the ear becomes swollen and puffy. The swelling can spread to the upper neck and jaw. In most patients, the swelling is found on both sides of the face. The swelling is rarely severe, but sometimes the patient may have trouble chewing and swallowing.
Complications from mumps are rare but they can occur, particularly in older children. In some cases the meninges, a tissue that covers parts of the nervous system, can become inflamed. This leads to a disease called meningitis. Other complications can involve other glands in the body.
Treatment
The main symptoms of mumps—the swollen cheeks and neck—begin to go away after four or five days. There is no specific treatment for mumps. Because it is so contagious, patients should stay home. They should also get plenty of rest. Most patients can return to school or work after the swelling and other symptoms have gone away. However, it is always best to ask a doctor about this.
Prevention
Once a person is infected with mumps, he or she cannot get the disease again. This is called immunity. Another way to gain immunity from mumps is to be vaccinated against the disease. The vaccine used to protect against mumps is very effective. The same vaccine also protects against measles and rubella (also called German measles). Children in the United States usually receive this vaccine twice before they start school.
In some countries the vaccine is not as easily available. Those countries suffer frequent epidemics. This means that the disease spreads to large numbers of people within a short period of time. Epidemics can spread across cities, states, and continents, and they can even spread around the world. It is very important to prevent diseases like mumps from spreading and becoming an epidemic. One way to prevent this is by vaccination. It is very important to discuss the mumps vaccine, and the disease itself, with a doctor.
How mumps is spread
The glands that are infected by the mumps virus normally produce saliva. Because of this, when a person is infected, pieces of the virus become mixed in with the saliva produced by the glands. Any contact with the saliva of an infected person can therefore spread the disease.When an infected person coughs or sneezes, tiny particles of the virus are spread into the air. If these are inhaled by an uninfected person or a person who has not been vaccinated against the disease, that person will become ill with mumps. The disease can also be spread by touching something, such as bedding, that has infected saliva on it.
Symptoms
Once a person is infected with the mumps virus, it usually takes two to three weeks for symptoms, or signs of the disease, to appear. The first symptoms a patient will feel are very general and resemble those of the flu. The patient may have a runny nose and a slight fever. Soon the area in front of the ear becomes swollen and puffy. The swelling can spread to the upper neck and jaw. In most patients, the swelling is found on both sides of the face. The swelling is rarely severe, but sometimes the patient may have trouble chewing and swallowing.
Complications from mumps are rare but they can occur, particularly in older children. In some cases the meninges, a tissue that covers parts of the nervous system, can become inflamed. This leads to a disease called meningitis. Other complications can involve other glands in the body.
Treatment
The main symptoms of mumps—the swollen cheeks and neck—begin to go away after four or five days. There is no specific treatment for mumps. Because it is so contagious, patients should stay home. They should also get plenty of rest. Most patients can return to school or work after the swelling and other symptoms have gone away. However, it is always best to ask a doctor about this.
Prevention
Once a person is infected with mumps, he or she cannot get the disease again. This is called immunity. Another way to gain immunity from mumps is to be vaccinated against the disease. The vaccine used to protect against mumps is very effective. The same vaccine also protects against measles and rubella (also called German measles). Children in the United States usually receive this vaccine twice before they start school.
In some countries the vaccine is not as easily available. Those countries suffer frequent epidemics. This means that the disease spreads to large numbers of people within a short period of time. Epidemics can spread across cities, states, and continents, and they can even spread around the world. It is very important to prevent diseases like mumps from spreading and becoming an epidemic. One way to prevent this is by vaccination. It is very important to discuss the mumps vaccine, and the disease itself, with a doctor.
Hodgkin disease
an uncommon cancer of the lymphatic system (malignant lymphoma) that usually strikes young adults and people 55 years of age or older. Most patients can be cured if the disease is detected in its early stages, but even those with advanced Hodgkin disease have a significant chance of recovery. The overall cure rate is approximately 75 percent.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
Saturday, May 17, 2008
Flu facts - tips and treatment
Influenza (the flu) is caused by a highly contagious virus, which is spread by coughs and sneezes. Flu epidemics occur when there are minor changes in the nature of the virus so that more people are susceptible.
Pandemics (worldwide epidemics) occur when there are major changes in the virus, and can cause very many deaths. There are three types of flu virus – A, B and C. Influenza A is more likely to cause epidemics.
Flu symptoms
Flu symptoms develop one to three days after infection and include:
* High fever, chills and sweating
* Sore throat
* Weakness
* Headache and generalised muscle and joint pains (legs and back) * A non-productive cough that can later become more severe and productive.
Flu versus the common cold
The flu is more than a bad cold.
* Cold symptoms last one to two days while the flu can last up to a week.
* The flu causes a high fever. A cold sometimes causes a mild fever.
* Muscular pains and shivering attacks occur with the flu but not with a cold.
* Colds cause a runny nose, while the flu usually starts with a dry sensation in the nose and throat.
Serious complications are rare
In a small proportion of cases, flu will lead to:
* Secondary bacterial pneumonia – occurs when bacteria invade the lungs. Symptoms include shortness of breath, green-yellow phlegm, chest pains and a temperature. Mortality rates are high but it is less lethal than primary influenza pneumonia.
* Primary influenza pneumonia – almost always results in death. Symptoms include difficulty breathing and blue discoloration of the skin (cyanosis).
* Inflammation of the brain or heart – can occur during recovery from the flu.
* Reye’s syndrome – leads to brain inflammation and liver degeneration and is fatal in between 10 and 40 per cent of cases. Children under 16 years should not be given any medication containing aspirin as it increases the risk of Reye’s syndrome.
People at risk of complications
Complications are more common among people with an underlying medical condition or reduced immunity. Flu can increase the risk of death or serious complications from the underlying disease.
Flu treatment
There are now specific antiviral drugs available, but their effectiveness is very limited. The recommended treatment for flu is:
* Stay in bed and rest until the temperature has been normal for 48 hours.
* Drink enough fluids to maintain normal urine output.
* Take paracetamol to control fever, aches and pains (adults can use aspirin). Early use of antiviral medication may shorten the length and severity of illness. Consult a doctor to discuss treatment.
* Avoid exposure to dust, alcohol, fumes and tobacco smoke as much as possible.
Consult a doctor if symptoms such as difficulty breathing, coughing up green-yellow phlegm or severe headache develop.
Flu immunisation is recommended for older and ‘at risk’ groups
Immunisation against the flu each year is recommended for:
* Everyone aged 65 years and older
* Koori and Torres Strait Islanders aged over 50
* Adults and children with chronic heart, lung or kidney disease or metabolic disorders such as diabetes
* Adults and children receiving immunosuppressive treatment (including long-term steroids)
* Residents in nursing homes or other long-term care facilities
* Persons with immune deficiency, including HIV
* People in contact with high-risk groups, including health care providers, staff of nursing homes and long-term care facilities, and anyone sharing a household with ‘at risk’ people including children six months or older.
In Australia, an annual influenza vaccine is recommended in March or April. Protection develops about two weeks after the injection and lasts for up to one year.
Where to get help
Your doctor
Your local council
Your local community health centre
Things to remember
* The flu is more than just a bad cold.
* Flu can occasionally lead to serious complications including death.
* Older and ‘at risk’ groups should be immunised every year against the flu.
* Protection after immunisation takes 10 to 14 days.
Pandemics (worldwide epidemics) occur when there are major changes in the virus, and can cause very many deaths. There are three types of flu virus – A, B and C. Influenza A is more likely to cause epidemics.
Flu symptoms
Flu symptoms develop one to three days after infection and include:
* High fever, chills and sweating
* Sore throat
* Weakness
* Headache and generalised muscle and joint pains (legs and back) * A non-productive cough that can later become more severe and productive.
Flu versus the common cold
The flu is more than a bad cold.
* Cold symptoms last one to two days while the flu can last up to a week.
* The flu causes a high fever. A cold sometimes causes a mild fever.
* Muscular pains and shivering attacks occur with the flu but not with a cold.
* Colds cause a runny nose, while the flu usually starts with a dry sensation in the nose and throat.
Serious complications are rare
In a small proportion of cases, flu will lead to:
* Secondary bacterial pneumonia – occurs when bacteria invade the lungs. Symptoms include shortness of breath, green-yellow phlegm, chest pains and a temperature. Mortality rates are high but it is less lethal than primary influenza pneumonia.
* Primary influenza pneumonia – almost always results in death. Symptoms include difficulty breathing and blue discoloration of the skin (cyanosis).
* Inflammation of the brain or heart – can occur during recovery from the flu.
* Reye’s syndrome – leads to brain inflammation and liver degeneration and is fatal in between 10 and 40 per cent of cases. Children under 16 years should not be given any medication containing aspirin as it increases the risk of Reye’s syndrome.
People at risk of complications
Complications are more common among people with an underlying medical condition or reduced immunity. Flu can increase the risk of death or serious complications from the underlying disease.
Flu treatment
There are now specific antiviral drugs available, but their effectiveness is very limited. The recommended treatment for flu is:
* Stay in bed and rest until the temperature has been normal for 48 hours.
* Drink enough fluids to maintain normal urine output.
* Take paracetamol to control fever, aches and pains (adults can use aspirin). Early use of antiviral medication may shorten the length and severity of illness. Consult a doctor to discuss treatment.
* Avoid exposure to dust, alcohol, fumes and tobacco smoke as much as possible.
Consult a doctor if symptoms such as difficulty breathing, coughing up green-yellow phlegm or severe headache develop.
Flu immunisation is recommended for older and ‘at risk’ groups
Immunisation against the flu each year is recommended for:
* Everyone aged 65 years and older
* Koori and Torres Strait Islanders aged over 50
* Adults and children with chronic heart, lung or kidney disease or metabolic disorders such as diabetes
* Adults and children receiving immunosuppressive treatment (including long-term steroids)
* Residents in nursing homes or other long-term care facilities
* Persons with immune deficiency, including HIV
* People in contact with high-risk groups, including health care providers, staff of nursing homes and long-term care facilities, and anyone sharing a household with ‘at risk’ people including children six months or older.
In Australia, an annual influenza vaccine is recommended in March or April. Protection develops about two weeks after the injection and lasts for up to one year.
Where to get help
Your doctor
Your local council
Your local community health centre
Things to remember
* The flu is more than just a bad cold.
* Flu can occasionally lead to serious complications including death.
* Older and ‘at risk’ groups should be immunised every year against the flu.
* Protection after immunisation takes 10 to 14 days.
Depression - teenagers
Young people can feel depressed for all sorts of reasons and their moods can vary, from feeling a bit blue to feeling overwhelming sadness and hopelessness. Some may even feel suicidal.
Around 20 per cent of teenagers experience depressive moods, but clinically significant depression in young people is often not recognised. Research shows that three per cent of Australians aged between three and 16 years have a depressive disorder each year.
Although it is often difficult to communicate with someone who is feeling low, it is important not to ignore a young person’s feelings. Knowing that family and friends care and are willing to give support can be the first vital step to getting better.
Different types of depressive disorders
The three main types of depressive disorders are:
* Depressed mood – feeling sad or blue is an emotion common to people of all ages. The feeling generally results from problems or loss. People usually feel better after talking about the problem or doing something they enjoy. A depressed mood doesn’t usually interfere with daily activities. This is part of human experience and not an illness.
* Dysthymia – a mild type of depression that can last for over a year in young people. They may lose interest in things they have enjoyed doing and appear down most of the time. They have less energy, find it difficult to concentrate and have trouble eating and sleeping. The most common factor is feeling bad about themselves and having less confidence and enjoyment in their lives. Dysthymia is much more serious than a depressed mood.
* Major depression – this illness is a change in the person from their usual self, which persists for at least two weeks. It may be triggered by a major stressful event, such as a death or broken relationship. Sometimes, however, it may have no obvious cause. Some of the symptoms and signs of major depression include severe sleeping problems, loss of enjoyment in usual activities, feeling hopeless or worthless, increasing drug and alcohol use, neglect of personal appearance, excessive worry about health, complaints about constant physical pains like headaches, carelessness about physical safety, behaviour problems and preoccupation with death and suicide.
Young people at risk
Depression can affect anyone, but some teenagers are more likely to become depressed if:
* They have a close relative who has suffered from depression
* They have had a major life stress or several stresses. A major life stress can be family break-up, school failure, bullying, experience of prejudice and social isolation because of sexual preferences, child abuse, loss of a parent, accident, broken relationship or moving to another area.
Suicide risk factors
Stresses that sound minor to adults may be very important to teenagers and should be taken seriously. Telling a teenager who is upset that their worry is ‘about nothing’ only makes things worse. They feel no one understands and this increases their sense of being alone in the world.
Things that may mean a teenager is seriously thinking about taking their life include:
* Talk or threats of suicide
* Hints such as ‘I won’t be a problem for you much longer’
* Previous attempts, especially if the person was alone at the time
* Careless risk-taking behaviour
* Sad or angry mood that doesn’t go away
* Giving away personal possessions
* Suddenly clearing out belongings and getting them in order
* Becoming suddenly cheerful without reason after being depressed.
Ways to help a depressed teenager
When teenagers are suffering with depression, they aren’t always able to ask for help and may even refuse your help at times. It is important that you:
* Take their depression seriously.
* Offer unconditional love and concern.
* Take time to listen when they want to talk about their feelings.
* Show them you are available without being ‘pushy’.
* Encourage them to do things you know they enjoy.
* Notice the little things they are doing that you approve of.
* Support and encourage your child to get help without nagging.
* If your child won’t go for help and you are worried, go by yourself first and get some advice on how to best handle the situation.
* Take seriously any talk about suicide and actions such as giving away special things – do whatever is needed to ensure their safety, even if it is against their wishes.
* Make sure you don’t keep a gun in your home.
Taking care of yourself
Parenting a teenager who is suffering depression can be very stressful. When you find yourself getting angry or frustrated:
* Take a step back and think about what is happening before reacting.
* Remember that your relationship with your child is important and they need it to continue.
* Think about your own views: are you wondering why you should have to put up with the terrible behaviour (which will only make the situation worse) or are you thinking, ‘Something must be wrong for my child to be behaving like this’ (which will lead to a search for the cause)?
* Ask people close to you for support.
* Ask someone the young person is close to (such as another relative) to help provide support, but make sure your child knows that you’re not rejecting them.
* Make sure you do things for yourself – you need to take care of your own needs if you are to help your child.
* Get professional help if you need to.
Professional help
There is a range of different treatments available for depression, including counselling and therapies. Antidepressant medications should be given with caution for young teenagers because of possible side effects. The right treatment depends on the individual needs and the situation of the teenager. It is important to persist until the right treatment is found, as young people are often particular about whom they will talk to.
Where to get help
* Your doctor
* Psychiatrist
* Counsellor
* Your local community health centre
* Find a GP near you who specialises in young people and mental health issues through the beyondblue website
* ReachOut!
Things to remember
* Depression in young people is often not recognised.
* Stresses that sound small to adults may be very important to teenagers and should be taken seriously.
* When teenagers are suffering with depression, they aren’t always able to ask for help and may even refuse your help at times.
* If your child won’t go for help and you are worried, go by yourself first to get advice on how to best handle the situation.
Around 20 per cent of teenagers experience depressive moods, but clinically significant depression in young people is often not recognised. Research shows that three per cent of Australians aged between three and 16 years have a depressive disorder each year.
Although it is often difficult to communicate with someone who is feeling low, it is important not to ignore a young person’s feelings. Knowing that family and friends care and are willing to give support can be the first vital step to getting better.
Different types of depressive disorders
The three main types of depressive disorders are:
* Depressed mood – feeling sad or blue is an emotion common to people of all ages. The feeling generally results from problems or loss. People usually feel better after talking about the problem or doing something they enjoy. A depressed mood doesn’t usually interfere with daily activities. This is part of human experience and not an illness.
* Dysthymia – a mild type of depression that can last for over a year in young people. They may lose interest in things they have enjoyed doing and appear down most of the time. They have less energy, find it difficult to concentrate and have trouble eating and sleeping. The most common factor is feeling bad about themselves and having less confidence and enjoyment in their lives. Dysthymia is much more serious than a depressed mood.
* Major depression – this illness is a change in the person from their usual self, which persists for at least two weeks. It may be triggered by a major stressful event, such as a death or broken relationship. Sometimes, however, it may have no obvious cause. Some of the symptoms and signs of major depression include severe sleeping problems, loss of enjoyment in usual activities, feeling hopeless or worthless, increasing drug and alcohol use, neglect of personal appearance, excessive worry about health, complaints about constant physical pains like headaches, carelessness about physical safety, behaviour problems and preoccupation with death and suicide.
Young people at risk
Depression can affect anyone, but some teenagers are more likely to become depressed if:
* They have a close relative who has suffered from depression
* They have had a major life stress or several stresses. A major life stress can be family break-up, school failure, bullying, experience of prejudice and social isolation because of sexual preferences, child abuse, loss of a parent, accident, broken relationship or moving to another area.
Suicide risk factors
Stresses that sound minor to adults may be very important to teenagers and should be taken seriously. Telling a teenager who is upset that their worry is ‘about nothing’ only makes things worse. They feel no one understands and this increases their sense of being alone in the world.
Things that may mean a teenager is seriously thinking about taking their life include:
* Talk or threats of suicide
* Hints such as ‘I won’t be a problem for you much longer’
* Previous attempts, especially if the person was alone at the time
* Careless risk-taking behaviour
* Sad or angry mood that doesn’t go away
* Giving away personal possessions
* Suddenly clearing out belongings and getting them in order
* Becoming suddenly cheerful without reason after being depressed.
Ways to help a depressed teenager
When teenagers are suffering with depression, they aren’t always able to ask for help and may even refuse your help at times. It is important that you:
* Take their depression seriously.
* Offer unconditional love and concern.
* Take time to listen when they want to talk about their feelings.
* Show them you are available without being ‘pushy’.
* Encourage them to do things you know they enjoy.
* Notice the little things they are doing that you approve of.
* Support and encourage your child to get help without nagging.
* If your child won’t go for help and you are worried, go by yourself first and get some advice on how to best handle the situation.
* Take seriously any talk about suicide and actions such as giving away special things – do whatever is needed to ensure their safety, even if it is against their wishes.
* Make sure you don’t keep a gun in your home.
Taking care of yourself
Parenting a teenager who is suffering depression can be very stressful. When you find yourself getting angry or frustrated:
* Take a step back and think about what is happening before reacting.
* Remember that your relationship with your child is important and they need it to continue.
* Think about your own views: are you wondering why you should have to put up with the terrible behaviour (which will only make the situation worse) or are you thinking, ‘Something must be wrong for my child to be behaving like this’ (which will lead to a search for the cause)?
* Ask people close to you for support.
* Ask someone the young person is close to (such as another relative) to help provide support, but make sure your child knows that you’re not rejecting them.
* Make sure you do things for yourself – you need to take care of your own needs if you are to help your child.
* Get professional help if you need to.
Professional help
There is a range of different treatments available for depression, including counselling and therapies. Antidepressant medications should be given with caution for young teenagers because of possible side effects. The right treatment depends on the individual needs and the situation of the teenager. It is important to persist until the right treatment is found, as young people are often particular about whom they will talk to.
Where to get help
* Your doctor
* Psychiatrist
* Counsellor
* Your local community health centre
* Find a GP near you who specialises in young people and mental health issues through the beyondblue website
* ReachOut!
Things to remember
* Depression in young people is often not recognised.
* Stresses that sound small to adults may be very important to teenagers and should be taken seriously.
* When teenagers are suffering with depression, they aren’t always able to ask for help and may even refuse your help at times.
* If your child won’t go for help and you are worried, go by yourself first to get advice on how to best handle the situation.
Friday, May 16, 2008
Agenesis Corpus Callosum
Description
Agenesis of the corpus callosum (ACC) is a rare congenital abnormality in which there is a partial or complete absence of the corpus callosum. This is the area of the brain which connects the two cerebral hemispheres.
In most patients, ACC is diagnosed within the first two years of life. It may occur as a severe syndrome in infancy or childhood, as a milder condition in young adults, or as an asymptomatic incidental finding. The first symptoms of ACC are usually seizures, which may be followed by feeding problems and delays in holding the head erect, sitting, standing, and walking. The seizures may be caused by a very common disorder called infantile spasms, which is associated with ACC. There may be impairments in mental and physical development, hand-eye coordination, and visual and auditory memory. Hydrocephalus may also occur. In mild cases, symptoms such as seizures, repetitive speech, or headaches may not appear for years.
ACC may occur as an isolated condition or in combination with other cerebral anomalies including Chiari Malformation and Dandy-Walker syndrome, Andermann syndrome (with progressive neuropathy), schizencephaly, holoprosencephaly, and migrational anomalies. Female children may also have a specific syndrome, called Aicardi syndrome, in which there is severe mental retardation and chorioretinal lacunae (lesions of the retina of the eye), in addition to ACC and infantile spasms.
ACC is also sometimes associated with complex multi-system malformations and with several chromosomal anomalies, including trisomy 13 and 18. There are non-nervous system malformations that may occur both with and without chromosomal aberrations such as midline facial defects.
Treatment
There is no standard course of treatment for ACC. Treatment usually involves management of symptoms such as hydrocephalus and seizures if they occur.
Prognosis
ACC does not cause death in the majority of patients. Although many children with the disorder will lead normal lives and have average intelligence, careful neuropsychological testing reveals subtle differences in higher cortical function compared to individuals of the same age and education without ACC. Children with ACC accompanied by developmental delay and/or seizure disorders should be screened for metabolic disorders. Mental retardation is non-progressive.
Agenesis of the corpus callosum (ACC) is a rare congenital abnormality in which there is a partial or complete absence of the corpus callosum. This is the area of the brain which connects the two cerebral hemispheres.
In most patients, ACC is diagnosed within the first two years of life. It may occur as a severe syndrome in infancy or childhood, as a milder condition in young adults, or as an asymptomatic incidental finding. The first symptoms of ACC are usually seizures, which may be followed by feeding problems and delays in holding the head erect, sitting, standing, and walking. The seizures may be caused by a very common disorder called infantile spasms, which is associated with ACC. There may be impairments in mental and physical development, hand-eye coordination, and visual and auditory memory. Hydrocephalus may also occur. In mild cases, symptoms such as seizures, repetitive speech, or headaches may not appear for years.
ACC may occur as an isolated condition or in combination with other cerebral anomalies including Chiari Malformation and Dandy-Walker syndrome, Andermann syndrome (with progressive neuropathy), schizencephaly, holoprosencephaly, and migrational anomalies. Female children may also have a specific syndrome, called Aicardi syndrome, in which there is severe mental retardation and chorioretinal lacunae (lesions of the retina of the eye), in addition to ACC and infantile spasms.
ACC is also sometimes associated with complex multi-system malformations and with several chromosomal anomalies, including trisomy 13 and 18. There are non-nervous system malformations that may occur both with and without chromosomal aberrations such as midline facial defects.
Treatment
There is no standard course of treatment for ACC. Treatment usually involves management of symptoms such as hydrocephalus and seizures if they occur.
Prognosis
ACC does not cause death in the majority of patients. Although many children with the disorder will lead normal lives and have average intelligence, careful neuropsychological testing reveals subtle differences in higher cortical function compared to individuals of the same age and education without ACC. Children with ACC accompanied by developmental delay and/or seizure disorders should be screened for metabolic disorders. Mental retardation is non-progressive.
Acoustic Neuroma
(Vestibular schwannoma, neurinoma)
Description
The eighth cranial nerve - also known as the auditory or vestibulocochlear nerve - consists of the vestibular and cochlear divisions, which runs from the inner ear to the brain. The cochlear division is responsible for transmitting information about hearing and vestibular division is responsible for balance.
An acoustic neuroma is a benign tumour that develops when the specialized (Schwann) cells surrounding the vestibular division of the auditory nerve, grow at an abnormal rate in the internal auditory canal. The tumour if left untreated, can grow into the auditory canal and all the way through to the brain.
Acoustic neuromas generally grow slowly, so symptoms develop gradually. The main ones - dizziness, hearing loss and ringing in the ears (tinnitus) - are due to the effects of the tumour pressing on the auditory nerve. If the tumour grows large enough, it also may press on the nearby facial nerve and cause facial paralysis or tingling. Although the tumors are not cancerous, they can become life threatening if they grow so large that they press on brain structures that control vital body functions.
People with a hereditary disease called neurofibromatosis have a higher risk of developing acoustic neuromas and can develop tumours on both sides of the head.
Because the tumour grows so slowly, the symptoms are easy to miss or misinterpret. The earliest and most common symptoms of an acoustic neuroma are a gradual reduction in hearing in one ear and tinnitus, a ringing or noisy sound in the ear.
Other possible symptoms that may occur, depending on the extent of the tumour, include: dizziness, loss of balance or clumsiness facial paralysis, numbness or tingling, headache, a feeling of something clogging the ear, or mental confusion.
Most of these tumours grow slowly, taking years before they become large enough to cause symptoms. Once diagnosed, they must be treated or carefully observed; they do not resolve on their own.
Treatment
Occasionally, doctors may recommend no action at all beyond regular monitoring. This is because an acoustic neuroma typically grows at a slow rate in the initial stages. However, in most cases, treatment is required. Options may include:
* Surgery – microsurgery techniques are used to remove the tumour. However, side effects can include loss of hearing, and facial nerve damage.
* Stereotactic procedure – a non-invasive device that directs gamma radiation at the tumour. Side effects may also be experienced with this procedure.
All patients will require close follow-up. Patients and their physicians need to pay close attention for hearing loss, balance and facial muscle weakness. Hearing tests and MRIs will be performed periodically to assess changes in growth or new growth.
Prognosis
Acoustic neuromas are not malignant and do not spread to other parts of the body.
However, some untreated neuromas can grow very aggressively and cause severe and permanent damage to nerves, ear and brain tissue. Hearing loss and balance problems related to the tumour may remain, even after treatment by surgery or radiation. If an acoustic neuroma is diagnosed early, when the tumour is small, treatment is more likely to preserve hearing.
Description
The eighth cranial nerve - also known as the auditory or vestibulocochlear nerve - consists of the vestibular and cochlear divisions, which runs from the inner ear to the brain. The cochlear division is responsible for transmitting information about hearing and vestibular division is responsible for balance.
An acoustic neuroma is a benign tumour that develops when the specialized (Schwann) cells surrounding the vestibular division of the auditory nerve, grow at an abnormal rate in the internal auditory canal. The tumour if left untreated, can grow into the auditory canal and all the way through to the brain.
Acoustic neuromas generally grow slowly, so symptoms develop gradually. The main ones - dizziness, hearing loss and ringing in the ears (tinnitus) - are due to the effects of the tumour pressing on the auditory nerve. If the tumour grows large enough, it also may press on the nearby facial nerve and cause facial paralysis or tingling. Although the tumors are not cancerous, they can become life threatening if they grow so large that they press on brain structures that control vital body functions.
People with a hereditary disease called neurofibromatosis have a higher risk of developing acoustic neuromas and can develop tumours on both sides of the head.
Because the tumour grows so slowly, the symptoms are easy to miss or misinterpret. The earliest and most common symptoms of an acoustic neuroma are a gradual reduction in hearing in one ear and tinnitus, a ringing or noisy sound in the ear.
Other possible symptoms that may occur, depending on the extent of the tumour, include: dizziness, loss of balance or clumsiness facial paralysis, numbness or tingling, headache, a feeling of something clogging the ear, or mental confusion.
Most of these tumours grow slowly, taking years before they become large enough to cause symptoms. Once diagnosed, they must be treated or carefully observed; they do not resolve on their own.
Treatment
Occasionally, doctors may recommend no action at all beyond regular monitoring. This is because an acoustic neuroma typically grows at a slow rate in the initial stages. However, in most cases, treatment is required. Options may include:
* Surgery – microsurgery techniques are used to remove the tumour. However, side effects can include loss of hearing, and facial nerve damage.
* Stereotactic procedure – a non-invasive device that directs gamma radiation at the tumour. Side effects may also be experienced with this procedure.
All patients will require close follow-up. Patients and their physicians need to pay close attention for hearing loss, balance and facial muscle weakness. Hearing tests and MRIs will be performed periodically to assess changes in growth or new growth.
Prognosis
Acoustic neuromas are not malignant and do not spread to other parts of the body.
However, some untreated neuromas can grow very aggressively and cause severe and permanent damage to nerves, ear and brain tissue. Hearing loss and balance problems related to the tumour may remain, even after treatment by surgery or radiation. If an acoustic neuroma is diagnosed early, when the tumour is small, treatment is more likely to preserve hearing.
Genital Herpes
Herpes simplex virus (HSV), better known as genital herpes, is a contagious viral infection estimated to infect 45 million Americans, with as many as 500,000 new cases occurring each year. Infections frequently go unrecognized by patients and/or clinicians. Two types of virus, HSV1 and HSV2, cause genital herpes. Both types produce sores in and around the vagina, penis, anal opening, and on the buttocks or thighs. Sores may also appear on other areas whenever broken skin comes into contact with HSV.
The virus invades nerves cells and can reside there for life, causing periodic symptoms. Genital herpes infection is acquired by sexual contact with a partner having an outbreak of herpes sores in the genital area. Oral herpes can be transmitted to the genital area of a partner during oral sex. Some herpes infections may make people more likely to get an HIV infection if exposed to the virus. Reliable tests for HSV antibodies are now readily available. In addition, PCR tests can be used to detect herpes infection.
Potent Fact
Genital herpes is not readily spread by contact with a toilet seat or in a hot tub.
There is no cure for herpes. However, there are a number of drugs that are effective in treating the herpes virus. Acyclovir, an antiviral drug, is the “gold standard” of therapy. These drugs reduce symptoms and help to speed healing. They also lessen the chances of outbreaks. There is no vaccine for genital herpes, although recent trials of vaccines reduced the risk of infection by 75 percent. The vaccine was not effective in men, however, making it the first time a vaccine worked in one sex and not in the other. Unfortunately, herpes can be spread even if the infection is inactive.
The virus invades nerves cells and can reside there for life, causing periodic symptoms. Genital herpes infection is acquired by sexual contact with a partner having an outbreak of herpes sores in the genital area. Oral herpes can be transmitted to the genital area of a partner during oral sex. Some herpes infections may make people more likely to get an HIV infection if exposed to the virus. Reliable tests for HSV antibodies are now readily available. In addition, PCR tests can be used to detect herpes infection.
Potent Fact
Genital herpes is not readily spread by contact with a toilet seat or in a hot tub.
There is no cure for herpes. However, there are a number of drugs that are effective in treating the herpes virus. Acyclovir, an antiviral drug, is the “gold standard” of therapy. These drugs reduce symptoms and help to speed healing. They also lessen the chances of outbreaks. There is no vaccine for genital herpes, although recent trials of vaccines reduced the risk of infection by 75 percent. The vaccine was not effective in men, however, making it the first time a vaccine worked in one sex and not in the other. Unfortunately, herpes can be spread even if the infection is inactive.
Tuberculosis
Introduction
In an age when we believe that we have the tools to conquer most diseases, the ancient scourge of tuberculosis (TB) still causes 2 million deaths a year worldwide—more than any other single infectious organism—reminding us that we still have a long way to go. Even equipped with drugs to treat TB effectively, we haven't managed to eradicate this deadly infection.
What is the history of tuberculosis? And how has it managed to survive for so long? This section will answer these questions, plus describe the symptoms and treatment options available for TB.
An Ancient Scourge That Still Kills Today
Mycobacterium tuberculosis, the bacteria that causes tuberculosis, has been around for centuries. Recently, fragments of the spinal columns from Egyptian mummies from 2400 B.C.E. were found to have definite signs of the ravages of this terrible disease. Also called consumption, TB was identified as the most widespread disease in ancient Greece, where it was almost always fatal. But it wasn't until centuries later that the first descriptions of the disease began to appear. Starting in the late seventeenth century, physicians began to identify changes in the lungs common in all consumptive, or TB, patients. At the same time, the earliest references to the fact that the disease was infectious began to appear.
In 1720, the English doctor Benjamin Marten was the first to state that TB could be caused by “wonderfully minute living creatures.” He went further to say that it was likely that ongoing contact with a consumptive patient could cause a healthy person to get sick. Although Marten's findings didn't help to cure TB, they did help people to better understand the disease.
The sanitorium, which was introduced in the mid-nineteenth century, was the first positive step to contain TB. Hermann Brehmer, a Silesian botany student who had TB, was told by his doctor to find a healthy climate. He moved to the Himalayas and continued his studies. He survived his bout with the illness, and after he received his doctorate, built an institution in Gorbersdorf, where TB patients could come to recuperate. They received good nutrition and were outside in fresh air most of the day. This became the model for the development of sanitoria around the world.
In 1865, French military doctor Jean-Antoine Villemin demonstrated that TB could be passed from people to cattle and from cattle to rabbits. In 1882, Robert Koch discovered a staining technique that allowed him to see the bacteria that cause TB under a microscope.
Until the introduction of surgical techniques to remove infected tissue and the development of x-rays to monitor the disease, doctors didn't have great tools to treat TB. TB patients could be isolated, which helped reduce the spread of the disease, but treating it remained a challenge.
Disease Diction
Tuberculosis was first formally described by Greek physician Hippocrates around 460 B.C.E. He called it phthsis which is the Greek word for consumption, because it described the way the disease consumed its victims. Consumption was the most widespread disease of the time, and most of its victims died. The word consumption was used to describe the disease until 1882, when the tuberculosis bacteria was identified as the cause of the disease.
Antigen Alert
Tuberculosis is spread through the air, so everyone is at some risk.
In an age when we believe that we have the tools to conquer most diseases, the ancient scourge of tuberculosis (TB) still causes 2 million deaths a year worldwide—more than any other single infectious organism—reminding us that we still have a long way to go. Even equipped with drugs to treat TB effectively, we haven't managed to eradicate this deadly infection.
What is the history of tuberculosis? And how has it managed to survive for so long? This section will answer these questions, plus describe the symptoms and treatment options available for TB.
An Ancient Scourge That Still Kills Today
Mycobacterium tuberculosis, the bacteria that causes tuberculosis, has been around for centuries. Recently, fragments of the spinal columns from Egyptian mummies from 2400 B.C.E. were found to have definite signs of the ravages of this terrible disease. Also called consumption, TB was identified as the most widespread disease in ancient Greece, where it was almost always fatal. But it wasn't until centuries later that the first descriptions of the disease began to appear. Starting in the late seventeenth century, physicians began to identify changes in the lungs common in all consumptive, or TB, patients. At the same time, the earliest references to the fact that the disease was infectious began to appear.
In 1720, the English doctor Benjamin Marten was the first to state that TB could be caused by “wonderfully minute living creatures.” He went further to say that it was likely that ongoing contact with a consumptive patient could cause a healthy person to get sick. Although Marten's findings didn't help to cure TB, they did help people to better understand the disease.
The sanitorium, which was introduced in the mid-nineteenth century, was the first positive step to contain TB. Hermann Brehmer, a Silesian botany student who had TB, was told by his doctor to find a healthy climate. He moved to the Himalayas and continued his studies. He survived his bout with the illness, and after he received his doctorate, built an institution in Gorbersdorf, where TB patients could come to recuperate. They received good nutrition and were outside in fresh air most of the day. This became the model for the development of sanitoria around the world.
In 1865, French military doctor Jean-Antoine Villemin demonstrated that TB could be passed from people to cattle and from cattle to rabbits. In 1882, Robert Koch discovered a staining technique that allowed him to see the bacteria that cause TB under a microscope.
Until the introduction of surgical techniques to remove infected tissue and the development of x-rays to monitor the disease, doctors didn't have great tools to treat TB. TB patients could be isolated, which helped reduce the spread of the disease, but treating it remained a challenge.
Disease Diction
Tuberculosis was first formally described by Greek physician Hippocrates around 460 B.C.E. He called it phthsis which is the Greek word for consumption, because it described the way the disease consumed its victims. Consumption was the most widespread disease of the time, and most of its victims died. The word consumption was used to describe the disease until 1882, when the tuberculosis bacteria was identified as the cause of the disease.
Antigen Alert
Tuberculosis is spread through the air, so everyone is at some risk.
Haemophilia
Haemophilia or hemophilia (from Greek haima "blood" and philia "to love") is the name of a family of hereditary genetic disorders that impair the body's ability to control blood clotting, or coagulation. In the most common form, hemophilia A, clotting factor VIII is absent. Haemophilia B, also known as factor IX deficiency, is the second most common type of hemophilia, but Hemophilia B is far less common than Hemophilia A, the latter occurring in about one in 25,000 male births.
The effects of this sex-linked, X chromosome disorder are manifested almost entirely in males, although the gene for the disorder is inherited from the mother. This is more common in males because the female has two X chromosomes while the male only has one, meaning that if a male's x chromosome is defective, there is not another to "cover up" the disorder like females have. Sometimes this disease is considered to be dominant because of its dominance in the male XY chromosome pair. In about 30% of cases of Hemopilia B, however, there is no family history of the disorder and the condition is the result of a spontaneous gene mutation. A mother who is a carrier also has a 50% chance of giving the faulty X chromosome to her daughter. That does not give the daughter the hemophilia disease, but it does result in the daughter becoming a hemophilia carrier. Females are almost exclusively asymptomatic carriers of the disorder, and may have inherited it from either their mother or father.
These genetic deficiencies may lower blood plasma clotting factor levels of coagulation factors needed for a normal clotting process. When a blood vessel is injured, a temporary scab does form, but the missing coagulation factors prevent fibrin formation which is necessary to maintain the blood clot. Thus a haemophiliac does not bleed more intensely than a normal person, but for a much longer amount of time. In severe haemophiliacs even a minor injury could result in blood loss lasting days, weeks, or not ever healing completely. The critical risk here is with normally small bleeds which due to missing factor VIII take long times to heal. In areas such as the brain or inside joints this can be fatal or life debilitating.
The bleeding with external injury is normal, but incidence of late re-bleeding and internal bleeding is increased, especially into muscles, joints, or bleeding into closed spaces. Major complications include hemarthrosis, hemorrhage, gastrointestinal bleeding, and menorrhagia.
Causes
It is caused by a lack of clotting factors:
* Hemophilia A involves a lack of functional clotting Factor VIII. (This represents 90% of haemophilia cases.[citation needed])
* Hemophilia B involves a lack of functional clotting Factor IX.
* Hemophilia C involves a lack of functional clotting Factor XI.
* Hypofibrinogenemia involves a lack of functional clotting factor Factor I. Because it is so rare, about 1 or 2 cases per million births, it has no definite treatment approved by the FDA. It affects males and females equally. The blood of people with Hypofibrinogenemia neither clots nor contains sufficient amounts of Fibrinogen.
History
The earliest possible implicit reference to hemophilia may have been in the Talmud[4], a Jewish holy text, which states that males did not have to be circumcised if two brothers had already died from the procedure. In 1000, the Arab physician Abu al-Qasim al-Zahrawi (known as Albucasis in the West) wrote a more explicit description of hemophilia in his Al-Tasrif, in which he wrote of an Andalusian family whose males died of bleeding after minor injuries.
In 1803, Dr. John Conrad Otto, a Philadelphia physician, wrote an account about "a hemorrhagic disposition existing in certain families." He recognized that the disorder was hereditary and that it affected males and rarely females. He was able to trace the disease back to a woman who settled near Plymouth in 1720. The first usage of the term "hemophilia" appears in a description of the condition written by Hopff at the University of Zurich in 1828. In 1937, Patek and Taylor, two doctors from Harvard, discovered anti-hemophilic globulin. Pavlosky, a doctor from Buenos Aires, found Hemophilia A and Hemophilia B to be separate diseases by doing a lab test. This test was done by transferring the blood of one hemophiliac to another hemophiliac. The fact that this corrected the clotting problem showed that there was more than one form of hemophilia.
Haemophilia in European royalty featured prominently and thus is sometimes known as "the royal disease". Queen Victoria passed the mutation to her son Leopold and, through several of her daughters, to various royals across the continent, including the royal families of Spain, Germany, and Russia. Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria and suffered from hemophilia.
Prior to 1985, there were no laws enacted within the U.S. to screen blood, even though the technology existed. As a result, many hemophilia patients who received untested and unscreened clotting factor prior to 1992 were at an extreme risk for contracting HIV and Hepatitis C via these blood products. It is estimated that more than 50% of the Hemophilia population, over 10,000 people, contracted HIV from the tainted blood supply in the United States alone.
About 18,000 people in the United States have hemophilia. Each year, about 400 babies are born with the disorder. Hemophilia usually occurs in males and less often in females.
Genetics

Females possess two X-chromosomes, whereas males have one X and one Y chromosome. Since the mutations causing the disease are recessive, a woman carrying the defect on one of her X-chromosomes may not be affected by it, as the equivalent allele on her other chromosome should express itself to produce the necessary clotting factors. However the Y-chromosome in men has no gene for factors VIII or IX. If the genes responsible for production of factor VIII or factor IX present on a male's X-chromosome are deficient there is no equivalent on the Y-chromosome, so the deficient gene is not masked by the dominant allele and he will develop the illness.
Since a male receives his single X-chromosome from his mother, the son of a healthy female silently carrying the deficient gene will have a 50% chance of inheriting that gene from her and with it the disease; and if his mother is affected with haemophilia, he will have a 100% chance of being a haemophiliac. In contrast, for a female to inherit the disease, she must receive two deficient X-chromosomes, one from her mother and the other from her father (who must therefore be a haemophiliac himself). Hence haemophilia is far more common among males than females. However it is possible for female carriers to become mild haemophiliacs due to lyonisation of the X chromosomes. Haemophiliac daughters are more common than they once were, as improved treatments for the disease have allowed more haemophiliac males to survive to adulthood and become parents. Adult females may experience menorrhagia (heavy periods) due to the bleeding tendency. The pattern of inheritance is criss-cross type. This type of pattern is also seen in colour blindness.
As with all genetic disorders, it is of course also possible for a human to acquire it spontaneously through mutation, rather than inheriting it, because of a new mutation in one of their parents' gametes. Spontaneous mutations account for about ⅓ of all haemophilia A and 20% of all hemophilia B cases. Genetic testing and genetic counseling is recommended for families with haemophilia. Prenatal testing, such as amniocentesis, is available to pregnant women who may be carriers of the condition.
Treatment
Though there is no cure for hemophilia, it can be controlled with regular infusions of the deficient clotting factor, i.e. factor VIII in haemophilia A or factor IX in hemophilia B. Some hemophiliacs develop antibodies (inhibitors) against the replacement factors given to them, so the amount of the factor has to be increased or non-human replacement products must be given, such as porcine factor VIII.
If a patient becomes refractory to replacement coagulation factor as a result of circulating inhibitors, this may be partially overcome with recombinant human factor VII (NovoSeven®), which is registered for this indication in many countries.
In early 2008, the US Food and Drug Administration approved Xyntha® (Wyeth) anti-hemophilic factor, genetically engineered from the genes of Chinese hamster ovary cells. Since 1993 (Dr. Mary Nugent) recombinant factor products (which are typically cultured in Chinese hamster ovary (CHO) tissue culture cells and involve little, if any human plasma products) have been available and have been widely used in wealthier western countries. While recombinant clotting factor products offer higher purity and safety, they are, like concentrate, extremely expensive, and not generally available in the developing world. In many cases, factor products of any sort are difficult to obtain in developing countries.
In Western countries, common standards of care fall into one of two categories: prophylaxis or on-demand. Prophylaxis involves the infusion of clotting factor on a regular schedule in order to keep clotting levels sufficiently high to prevent spontaneous bleeding episodes. On-demand treatment involves treating bleeding episodes once they arise. In 2007, a clinical trial was published in the New England Journal of Medicine (NEJM) comparing on-demand treatment of boys (< 30 months) with Hemophilia A with prophylactic treatment (infusions of 25 IU/kg body weight of Factor VIII every other day) in respect to its effect on the prevention of joint-diseases. When the boys reached 6 years of age, 93% of those in the prophylaxis group and 55% of those in the episodic-therapy group had a normal index joint-structure on MRI. Prophylactic treatment, however, resulted in average costs of $300,000 per year. The author of an editorial published in the same issue of the NEJM demands more clinical studies addressing the cost-effectiveness of prophylactic treatment.
Armour and other pharmaceutical companies knowingly sold blood clotting products contaminated with HIV and hepatitis C to ten thousand hemophiliacs across America in the late 1970's and early mid 1980's. When the Federal Government banned their products from being sold in America, they promptly turned around and sold the HIV contaminated factor products overseas in Europe and Japan.
Later criminal and civil lawsuits were brought against these manufacturers and the Armour Pharmaceutical subsidiary of French chemical company Rhone-Poulenc. In Europe and Japan several high level executives received prison terms as a result of their knowingly selling HIV contaminated products to hemophiliacs.
In America the pharmaceutical companies eventually paid out around 650 million dollars to compensate the haemophiliacs who were infected with HIV. [12]
As a direct result of the contamination of the blood supply in the late 1970s and early/mid 1980s with viruses such as Hepatitis and HIV, new methods were developed in the production of clotting factor products. The initial response was to heat-treat (pasteurize) plasma-derived factor concentrate, followed by the development of monoclonal factor concentrates, which use a combination of heat treatment and affinity chromatography to inactivate any viral agents in the pooled plasma from which the factor concentrate is derived. The Lindsay Tribunal in Ireland investigated, among other things, the slow adoption of the new methods.
It was claimed that Rasputin was successful at treating the Tsarevich Alexei of Russia's hemophilia. At the time, a common treatment administered by professional doctors was to use aspirin, which worsened rather than lessen the problem. It is believe that, by simply advising against the medical treatment, Rasputin could bring visible and significant improvement to the condition of Alexei.
People affected with Hemophilia are recommended to do some specific exercises for elbow, knee, and ankles like stretching of calves, ankle circles, elbow flexion, and Quadriceps set etc. These exercises are recommended after an internal bleed occurs and on a daily basis to strengthen the muscles and joints to prevent new bleeding problems.
The effects of this sex-linked, X chromosome disorder are manifested almost entirely in males, although the gene for the disorder is inherited from the mother. This is more common in males because the female has two X chromosomes while the male only has one, meaning that if a male's x chromosome is defective, there is not another to "cover up" the disorder like females have. Sometimes this disease is considered to be dominant because of its dominance in the male XY chromosome pair. In about 30% of cases of Hemopilia B, however, there is no family history of the disorder and the condition is the result of a spontaneous gene mutation. A mother who is a carrier also has a 50% chance of giving the faulty X chromosome to her daughter. That does not give the daughter the hemophilia disease, but it does result in the daughter becoming a hemophilia carrier. Females are almost exclusively asymptomatic carriers of the disorder, and may have inherited it from either their mother or father.
These genetic deficiencies may lower blood plasma clotting factor levels of coagulation factors needed for a normal clotting process. When a blood vessel is injured, a temporary scab does form, but the missing coagulation factors prevent fibrin formation which is necessary to maintain the blood clot. Thus a haemophiliac does not bleed more intensely than a normal person, but for a much longer amount of time. In severe haemophiliacs even a minor injury could result in blood loss lasting days, weeks, or not ever healing completely. The critical risk here is with normally small bleeds which due to missing factor VIII take long times to heal. In areas such as the brain or inside joints this can be fatal or life debilitating.
The bleeding with external injury is normal, but incidence of late re-bleeding and internal bleeding is increased, especially into muscles, joints, or bleeding into closed spaces. Major complications include hemarthrosis, hemorrhage, gastrointestinal bleeding, and menorrhagia.
Causes
It is caused by a lack of clotting factors:
* Hemophilia A involves a lack of functional clotting Factor VIII. (This represents 90% of haemophilia cases.[citation needed])
* Hemophilia B involves a lack of functional clotting Factor IX.
* Hemophilia C involves a lack of functional clotting Factor XI.
* Hypofibrinogenemia involves a lack of functional clotting factor Factor I. Because it is so rare, about 1 or 2 cases per million births, it has no definite treatment approved by the FDA. It affects males and females equally. The blood of people with Hypofibrinogenemia neither clots nor contains sufficient amounts of Fibrinogen.
History
The earliest possible implicit reference to hemophilia may have been in the Talmud[4], a Jewish holy text, which states that males did not have to be circumcised if two brothers had already died from the procedure. In 1000, the Arab physician Abu al-Qasim al-Zahrawi (known as Albucasis in the West) wrote a more explicit description of hemophilia in his Al-Tasrif, in which he wrote of an Andalusian family whose males died of bleeding after minor injuries.
In 1803, Dr. John Conrad Otto, a Philadelphia physician, wrote an account about "a hemorrhagic disposition existing in certain families." He recognized that the disorder was hereditary and that it affected males and rarely females. He was able to trace the disease back to a woman who settled near Plymouth in 1720. The first usage of the term "hemophilia" appears in a description of the condition written by Hopff at the University of Zurich in 1828. In 1937, Patek and Taylor, two doctors from Harvard, discovered anti-hemophilic globulin. Pavlosky, a doctor from Buenos Aires, found Hemophilia A and Hemophilia B to be separate diseases by doing a lab test. This test was done by transferring the blood of one hemophiliac to another hemophiliac. The fact that this corrected the clotting problem showed that there was more than one form of hemophilia.
Haemophilia in European royalty featured prominently and thus is sometimes known as "the royal disease". Queen Victoria passed the mutation to her son Leopold and, through several of her daughters, to various royals across the continent, including the royal families of Spain, Germany, and Russia. Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria and suffered from hemophilia.
Prior to 1985, there were no laws enacted within the U.S. to screen blood, even though the technology existed. As a result, many hemophilia patients who received untested and unscreened clotting factor prior to 1992 were at an extreme risk for contracting HIV and Hepatitis C via these blood products. It is estimated that more than 50% of the Hemophilia population, over 10,000 people, contracted HIV from the tainted blood supply in the United States alone.
About 18,000 people in the United States have hemophilia. Each year, about 400 babies are born with the disorder. Hemophilia usually occurs in males and less often in females.
Genetics
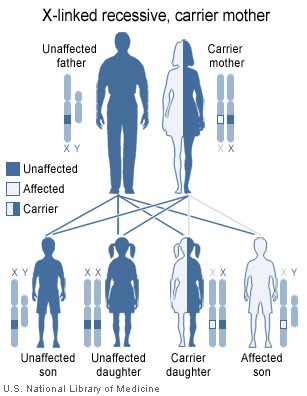
Females possess two X-chromosomes, whereas males have one X and one Y chromosome. Since the mutations causing the disease are recessive, a woman carrying the defect on one of her X-chromosomes may not be affected by it, as the equivalent allele on her other chromosome should express itself to produce the necessary clotting factors. However the Y-chromosome in men has no gene for factors VIII or IX. If the genes responsible for production of factor VIII or factor IX present on a male's X-chromosome are deficient there is no equivalent on the Y-chromosome, so the deficient gene is not masked by the dominant allele and he will develop the illness.
Since a male receives his single X-chromosome from his mother, the son of a healthy female silently carrying the deficient gene will have a 50% chance of inheriting that gene from her and with it the disease; and if his mother is affected with haemophilia, he will have a 100% chance of being a haemophiliac. In contrast, for a female to inherit the disease, she must receive two deficient X-chromosomes, one from her mother and the other from her father (who must therefore be a haemophiliac himself). Hence haemophilia is far more common among males than females. However it is possible for female carriers to become mild haemophiliacs due to lyonisation of the X chromosomes. Haemophiliac daughters are more common than they once were, as improved treatments for the disease have allowed more haemophiliac males to survive to adulthood and become parents. Adult females may experience menorrhagia (heavy periods) due to the bleeding tendency. The pattern of inheritance is criss-cross type. This type of pattern is also seen in colour blindness.
As with all genetic disorders, it is of course also possible for a human to acquire it spontaneously through mutation, rather than inheriting it, because of a new mutation in one of their parents' gametes. Spontaneous mutations account for about ⅓ of all haemophilia A and 20% of all hemophilia B cases. Genetic testing and genetic counseling is recommended for families with haemophilia. Prenatal testing, such as amniocentesis, is available to pregnant women who may be carriers of the condition.
Treatment
Though there is no cure for hemophilia, it can be controlled with regular infusions of the deficient clotting factor, i.e. factor VIII in haemophilia A or factor IX in hemophilia B. Some hemophiliacs develop antibodies (inhibitors) against the replacement factors given to them, so the amount of the factor has to be increased or non-human replacement products must be given, such as porcine factor VIII.
If a patient becomes refractory to replacement coagulation factor as a result of circulating inhibitors, this may be partially overcome with recombinant human factor VII (NovoSeven®), which is registered for this indication in many countries.
In early 2008, the US Food and Drug Administration approved Xyntha® (Wyeth) anti-hemophilic factor, genetically engineered from the genes of Chinese hamster ovary cells. Since 1993 (Dr. Mary Nugent) recombinant factor products (which are typically cultured in Chinese hamster ovary (CHO) tissue culture cells and involve little, if any human plasma products) have been available and have been widely used in wealthier western countries. While recombinant clotting factor products offer higher purity and safety, they are, like concentrate, extremely expensive, and not generally available in the developing world. In many cases, factor products of any sort are difficult to obtain in developing countries.
In Western countries, common standards of care fall into one of two categories: prophylaxis or on-demand. Prophylaxis involves the infusion of clotting factor on a regular schedule in order to keep clotting levels sufficiently high to prevent spontaneous bleeding episodes. On-demand treatment involves treating bleeding episodes once they arise. In 2007, a clinical trial was published in the New England Journal of Medicine (NEJM) comparing on-demand treatment of boys (< 30 months) with Hemophilia A with prophylactic treatment (infusions of 25 IU/kg body weight of Factor VIII every other day) in respect to its effect on the prevention of joint-diseases. When the boys reached 6 years of age, 93% of those in the prophylaxis group and 55% of those in the episodic-therapy group had a normal index joint-structure on MRI. Prophylactic treatment, however, resulted in average costs of $300,000 per year. The author of an editorial published in the same issue of the NEJM demands more clinical studies addressing the cost-effectiveness of prophylactic treatment.
Armour and other pharmaceutical companies knowingly sold blood clotting products contaminated with HIV and hepatitis C to ten thousand hemophiliacs across America in the late 1970's and early mid 1980's. When the Federal Government banned their products from being sold in America, they promptly turned around and sold the HIV contaminated factor products overseas in Europe and Japan.
Later criminal and civil lawsuits were brought against these manufacturers and the Armour Pharmaceutical subsidiary of French chemical company Rhone-Poulenc. In Europe and Japan several high level executives received prison terms as a result of their knowingly selling HIV contaminated products to hemophiliacs.
In America the pharmaceutical companies eventually paid out around 650 million dollars to compensate the haemophiliacs who were infected with HIV. [12]
As a direct result of the contamination of the blood supply in the late 1970s and early/mid 1980s with viruses such as Hepatitis and HIV, new methods were developed in the production of clotting factor products. The initial response was to heat-treat (pasteurize) plasma-derived factor concentrate, followed by the development of monoclonal factor concentrates, which use a combination of heat treatment and affinity chromatography to inactivate any viral agents in the pooled plasma from which the factor concentrate is derived. The Lindsay Tribunal in Ireland investigated, among other things, the slow adoption of the new methods.
It was claimed that Rasputin was successful at treating the Tsarevich Alexei of Russia's hemophilia. At the time, a common treatment administered by professional doctors was to use aspirin, which worsened rather than lessen the problem. It is believe that, by simply advising against the medical treatment, Rasputin could bring visible and significant improvement to the condition of Alexei.
People affected with Hemophilia are recommended to do some specific exercises for elbow, knee, and ankles like stretching of calves, ankle circles, elbow flexion, and Quadriceps set etc. These exercises are recommended after an internal bleed occurs and on a daily basis to strengthen the muscles and joints to prevent new bleeding problems.
Hepatitis
Hepatitis (plural hepatitides) implies injury to liver characterised by presence of inflammatory cells in the liver tissue. Etymologically from ancient Greek hepar (ηπαρ) or hepato- (ηπατο-) meaning 'liver' and suffix -itis denoting 'inflammation' (c.1727[1]). The condition can be self limiting, healing on its own or can progress to scarring of the liver. Hepatitis is acute when it lasts less than 6 months and chronic when it persists longer. A group of viruses known as the hepatitis viruses cause most cases of liver damage worldwide. Hepatitis can also be due to toxins (notably alcohol), other infections or from autoimmune process. It may run a subclinical course when the affected person may not feel ill. The patient becomes unwell and symptomatic when the disease impairs liver functions that include, among other things, screening of harmful substances, regulation of blood composition, and production of bile to help digestion.
Causes
Acute hepatitis
* Viral Hepatitis: Hepatitis A to E (more than 95% of viral cause), Herpes simplex, Cytomegalovirus, Epstein-Barr, yellow fever virus, adenoviruses.
* Non viral infection: toxoplasma, Leptospira, Q fever,[2] rocky mountain spotted fever[3]
* Alcohol
* Toxins: Amanita toxin in mushrooms, Carbon tetrachloride, asafetida
* Drugs: Paracetamol, amoxycillin, anti tuberculosis medicines, minocycline and many others (see longer list below).
* Ischemic hepatitis (circulatory insufficiency)
* Pregnancy
* Auto immune conditions e.g. Systemic Lupus Erythematosus (SLE)
* Metabolic diseases e.g. Wilson's disease
Chronic hepatitis
* Viral Hepatitis: Hepatitis B with or without hepatitis D, Hepatitis C (Hepatitis A and E do not lead to chronic disease)
* Autoimmune: Autoimmune hepatitis
* Alcohol
* Drugs: methyl-dopa, nitrofurantoin, isoniazide, ketoconazole
* Non-alcoholic steatohepatitis
* Heredity: Wilson's disease, alpha 1-antitrypsin deficiency
* Primary biliary cirrhosis and primary sclerosing cholangitis occasionally mimic chronic hepatitis
Signs and symptoms
Acute Hepatitis
Clinically, the course of acute hepatitis varies widely from mild symptoms requiring no treatment to fulminant hepatic failure needing liver transplantation. Acute viral hepatitis are more likely to be asymptomatic in younger people. Symptomatic individuals may present after convalescent stage of 7 to 10 days, with the total illness lasting 2 to 6 weeks.[4]
Initial features are of nonspecific flu-like symptoms, common to almost all acute viral infections and may include malaise, muscle and joint aches, fever, nausea or vomiting, diarrhea, and headache. More specific symptoms, which can be present in acute hepatitis from any cause are: profound loss of appetite, aversion to smoking among smokers, dark urine, yellowing of the eyes and skin (i.e. jaundice) and abdominal discomfort. Physical findings are usually minimal, apart from jaundice (33%) and tender hepatomegaly (10%). There can be occasional lymphadenopathy (5%) or splenomegaly (5%).[5]
Chronic Hepatitis
Majority of patients will remain asymptomatic or mildly symptomatic, abnormal blood tests being the only manifestation. Features may be related to extent of liver damage or the cause of hepatitis. Many experience return of symptoms related to acute hepatitis. Jaundice can be a late feature and may indicate extensive damage. Other features include abdominal fullness from enlarged liver or spleen, low grade fever and fluid retention (ascites). Extensive damage and scarring of liver i.e. cirrhosis leads to weight loss, easy bruising and bleeding tendencies. Acne, abnormal menstruation, lung scarring, inflammation of the thyroid gland and kidneys may be present in women with autoimmune hepatitis.[6]
Findings on clinical examination are usually those of cirrhosis or are related to aetiology.
Causes
Acute hepatitis
* Viral Hepatitis: Hepatitis A to E (more than 95% of viral cause), Herpes simplex, Cytomegalovirus, Epstein-Barr, yellow fever virus, adenoviruses.
* Non viral infection: toxoplasma, Leptospira, Q fever,[2] rocky mountain spotted fever[3]
* Alcohol
* Toxins: Amanita toxin in mushrooms, Carbon tetrachloride, asafetida
* Drugs: Paracetamol, amoxycillin, anti tuberculosis medicines, minocycline and many others (see longer list below).
* Ischemic hepatitis (circulatory insufficiency)
* Pregnancy
* Auto immune conditions e.g. Systemic Lupus Erythematosus (SLE)
* Metabolic diseases e.g. Wilson's disease
Chronic hepatitis
* Viral Hepatitis: Hepatitis B with or without hepatitis D, Hepatitis C (Hepatitis A and E do not lead to chronic disease)
* Autoimmune: Autoimmune hepatitis
* Alcohol
* Drugs: methyl-dopa, nitrofurantoin, isoniazide, ketoconazole
* Non-alcoholic steatohepatitis
* Heredity: Wilson's disease, alpha 1-antitrypsin deficiency
* Primary biliary cirrhosis and primary sclerosing cholangitis occasionally mimic chronic hepatitis
Signs and symptoms
Acute Hepatitis
Clinically, the course of acute hepatitis varies widely from mild symptoms requiring no treatment to fulminant hepatic failure needing liver transplantation. Acute viral hepatitis are more likely to be asymptomatic in younger people. Symptomatic individuals may present after convalescent stage of 7 to 10 days, with the total illness lasting 2 to 6 weeks.[4]
Initial features are of nonspecific flu-like symptoms, common to almost all acute viral infections and may include malaise, muscle and joint aches, fever, nausea or vomiting, diarrhea, and headache. More specific symptoms, which can be present in acute hepatitis from any cause are: profound loss of appetite, aversion to smoking among smokers, dark urine, yellowing of the eyes and skin (i.e. jaundice) and abdominal discomfort. Physical findings are usually minimal, apart from jaundice (33%) and tender hepatomegaly (10%). There can be occasional lymphadenopathy (5%) or splenomegaly (5%).[5]
Chronic Hepatitis
Majority of patients will remain asymptomatic or mildly symptomatic, abnormal blood tests being the only manifestation. Features may be related to extent of liver damage or the cause of hepatitis. Many experience return of symptoms related to acute hepatitis. Jaundice can be a late feature and may indicate extensive damage. Other features include abdominal fullness from enlarged liver or spleen, low grade fever and fluid retention (ascites). Extensive damage and scarring of liver i.e. cirrhosis leads to weight loss, easy bruising and bleeding tendencies. Acne, abnormal menstruation, lung scarring, inflammation of the thyroid gland and kidneys may be present in women with autoimmune hepatitis.[6]
Findings on clinical examination are usually those of cirrhosis or are related to aetiology.
Myocardial infarction
Acute myocardial infarction (AMI or MI), more commonly known as a heart attack, is a medical condition that occurs when the blood supply to a part of the heart is interrupted, most commonly due to rupture of a vulnerable plaque. The resulting ischemia or oxygen shortage causes damage and potential death of heart tissue. It is a medical emergency, and the leading cause of death for both men and women all over the world.[1] Important risk factors are a history of vascular disease such as atherosclerotic coronary heart disease and/or angina, a previous heart attack or stroke, any previous episodes of abnormal heart rhythms or syncope, older age—especially men over 40 and women over 50, smoking, excessive alcohol consumption, the abuse of certain drugs, high triglyceride levels, high LDL (low-density lipoprotein, "bad cholesterol") and low HDL (high density lipoprotein, "good cholesterol"), diabetes, high blood pressure, obesity, and chronically high levels of stress. Chronic kidney disease[2] and a history of heart failure[3] are also significant risk factors which may also predict fatality from MI.
The term myocardial infarction is derived from myocardium (the heart muscle) and infarction (tissue death due to oxygen starvation). The phrase "heart attack" is sometimes used incorrectly to describe sudden cardiac death, which may or may not be the result of acute myocardial infarction. A heart attack is different from, but can be the cause of cardiac arrest, which is the stopping of the heartbeat, and cardiac arrhythmia, an abnormal heartbeat.
Classical symptoms of acute myocardial infarction include chest pain (typically radiating to the left arm or left side of the neck), shortness of breath, nausea, vomiting, palpitations, sweating, and anxiety (often described as a sense of impending doom). Patients frequently feel suddenly ill. Women often experience different symptoms from men. The most common symptoms of MI in women include shortness of breath, weakness, and fatigue. Approximately one third of all myocardial infarctions are silent, without chest pain or other symptoms. A history of diabetes should heighten the index of suspicion, particularly if the patient has diabetic neuropathy (diabetes-related nerve damage).
Immediate treatment for suspected acute myocardial infarction includes oxygen, aspirin, and sublingual glyceryl trinitrate (colloquially referred to as nitroglycerin and abbreviated as NTG). pain relief is also often given, classically morphine sulfate.
The patient will receive a number of diagnostic tests, such as an electrocardiogram (ECG, EKG), a chest X-ray and blood tests to detect elevations in the creatine kinase-MB (CK-MB) fraction or in troponin I (TnI) or troponin T (TnT) levels (these are chemical markers specific to the myocardium and are often referred to as cardiac markers). On the basis of the ECG, a distinction is made between ST elevation MI (STEMI) or non-ST elevation MI (NSTEMI). Most cases of STEMI are treated with thrombolysis or if possible with percutaneous coronary intervention (PCI, angioplasty and stent insertion), provided the hospital has facilities for coronary angiography. NSTEMI is managed with medication, although PCI is often performed during hospital admission. In patients who have multiple blockages and who are relatively stable, or in a few extraordinary emergency cases, bypass surgery of the blocked coronary artery performed by a cardiothoracic surgeon is an option. Once admitted to hospital, the patient is observed on a coronary care unit, as the incidence of sustained ventricular tachycardia or ventricular fibrillation in the case of MI is high. In cases where the patient is unstable, more intensive nursing care may be warranted.
The term myocardial infarction is derived from myocardium (the heart muscle) and infarction (tissue death due to oxygen starvation). The phrase "heart attack" is sometimes used incorrectly to describe sudden cardiac death, which may or may not be the result of acute myocardial infarction. A heart attack is different from, but can be the cause of cardiac arrest, which is the stopping of the heartbeat, and cardiac arrhythmia, an abnormal heartbeat.
Classical symptoms of acute myocardial infarction include chest pain (typically radiating to the left arm or left side of the neck), shortness of breath, nausea, vomiting, palpitations, sweating, and anxiety (often described as a sense of impending doom). Patients frequently feel suddenly ill. Women often experience different symptoms from men. The most common symptoms of MI in women include shortness of breath, weakness, and fatigue. Approximately one third of all myocardial infarctions are silent, without chest pain or other symptoms. A history of diabetes should heighten the index of suspicion, particularly if the patient has diabetic neuropathy (diabetes-related nerve damage).
Immediate treatment for suspected acute myocardial infarction includes oxygen, aspirin, and sublingual glyceryl trinitrate (colloquially referred to as nitroglycerin and abbreviated as NTG). pain relief is also often given, classically morphine sulfate.
The patient will receive a number of diagnostic tests, such as an electrocardiogram (ECG, EKG), a chest X-ray and blood tests to detect elevations in the creatine kinase-MB (CK-MB) fraction or in troponin I (TnI) or troponin T (TnT) levels (these are chemical markers specific to the myocardium and are often referred to as cardiac markers). On the basis of the ECG, a distinction is made between ST elevation MI (STEMI) or non-ST elevation MI (NSTEMI). Most cases of STEMI are treated with thrombolysis or if possible with percutaneous coronary intervention (PCI, angioplasty and stent insertion), provided the hospital has facilities for coronary angiography. NSTEMI is managed with medication, although PCI is often performed during hospital admission. In patients who have multiple blockages and who are relatively stable, or in a few extraordinary emergency cases, bypass surgery of the blocked coronary artery performed by a cardiothoracic surgeon is an option. Once admitted to hospital, the patient is observed on a coronary care unit, as the incidence of sustained ventricular tachycardia or ventricular fibrillation in the case of MI is high. In cases where the patient is unstable, more intensive nursing care may be warranted.
Phobias known so far !!!
There are many hundreds of named phobias, and this is the most complete list of which we know.
Although there are many hundreds of 'different' phobias, all phobias are in fact very similar: a particular stimulus, be it spiders, snakes, or pretty well anything else triggering the phobic individuals fear response when it isn't appropriate.
The Phobia List: A
Ablutophobia — Fear of washing, bathing, or cleaning
Acarophobia — Fear of itching or the insects that cause itching
Acerophobia — Fear of sourness or things that are sour
Achluophobia — Fear of darkness or the dark
Acousticophobia — Fear of noise or sound
Acrophobia — Fear of heights or high levels
Aeroacrophobia — Fear of open high places
Aeronausiphobia — Fear of vomiting secondary to airsickness
Aerophobia — Fear of draft, swallowing air, or airbourne noxious substances
Agateophobia — Fear of insanity or becoming insane
Agliophobia — Fear of pain
Agoraphobia — Fear of open spaces, leaving a safe place, or crowded public places
Agraphobia — Fear of sexual abuse
Agrizoophobia — Fear of wild animals
Agyrophobia — Fear of streets or crossing the street
Aichmophobia — Fear of needles, pins, or pointed objects
Ailurophobia — Fear of cats
Albuminurophobia — Fear of kidney disease
Alektorophobia — Fear of chickens
Algophobia — Fear of garlic
Alliumphobia — Fear of opinions or beliefs
Altophobia — Fear of dust
Amathophobia — Fear of riding in cars
Amaxophobia — Fear of walking
Amnesiphobia — Fear of amnesia
Amychophobia — Fear of scratches or being scratched
Anablephobia — Fear of looking up
Androphobia — Fear of men
Anemophobia — Fear of wind or air drafts
Anginophobia — Fear of angina, choking, or narrowness
Anglophobia — Fear of England, English Culture, or English People
Angrophobia — Fear of anger or becoming angry
Ankylophobia — Fear of immobility of a joint
Anthophobia — Fear of flowers
Anthropophobia — Fear of people or society
Antlophobia — Fear of floods
Anuptaphobia — Fear of staying single
Anxiety — Fear of Anxiety
Apeirophobia — Fear of infinity
Aphenphosmphobia — Fear of being touched
Apiphobia — Fear of bees
Apotemnophobia — Fear of persons with amputations
Arachibutyrophobia — Fear of peanut butter sticking to the roof of the mouth
Arachnephobia — Fear of spiders
Arithmophobia — Fear of numbers
Arsonphobia — Fear of fire or flames
Asthenophobia — Fear of fainting or weakness
Astraphobia — Fear of thunder and lightning
Astrophobia — Fear of stars and celestial space
Asymmetriphobia — Fear of asymmetrical things
Ataxiophobia — Fear of ataxia (muscular incoordination)
Ataxophobia — Fear of disorder or untidiness
Atelophobia — Fear of imperfection
Atephobia — Fear of ruin or ruins
Athazagoraphobia — Fear of being forgotton, being ignored, or forgetting
Atomosophobia — Fear of atomic explosions
Atychiphobia — Fear of failure
Aulophobia — Fear of flutes
Aurophobia — Fear of gold
Auroraphobia — Fear of Northern lights
Autodysomophobia — Fear of one that has a vile odor
Automatonophobia — Fear of ventriloquist's dummies, animatronic creatures or wax statues
Automysophobia — Fear of being dirty
Autophobia — Fear of solitude, being alone, oneself, or being by oneself
Aviophobia — Fear of flying
The Phobia List: B
Bacillophobia — Fear of microbes
Bacteriophobia — Fear of bacteria
Ballistophobia — Fear of missiles or bullets
Barophobia — Fear of gravity
Basiphobia — Fear of inability to stand or falling
Bathmophobia — Fear of stairs or steep slopes
Bathophobia — Fear of depth
Batophobia — Fear of heights or being close to high buildings
Batrachophobia — Fear of amphibians, frogs, newts, or salamanders
Bibliophobia — Fear of books
Blennophobia — Fear of slime
Body Dysmorphic Disorder — Fear of having ugly or unattractive features
Bogyphobia — Fear of bogies or the bogeyman
Bolshephobia — Fear of Bolsheviks
Botanophobia — Fear of plants
Bromidrophobia — Fear of bodily odor or bodily smell
Bufonophobia — Fear of toads
The Phobia List: C
Cacophobia — Fear of ugliness or things that are ugly
Cainophobia — Fear of newness or novelty
Caligynephobia — Fear of beautiful women
Cancerophobia — Fear of cancer
Cardiophobia — Fear of the heart
Carnophobia — Fear of meat
Catagelophobia — Fear of being ridiculed or ridicule
Catapedaphobia — Fear of jumping from high and low places
Cathisophobia — Fear of sitting
Catoptrophobia — Fear of mirrors
Cheimaphobia — Fear of cold
Chemophobia — Fear of chemicals or working with chemicals
Cherophobia — Fear of gaiety
Chionophobia — Fear of snow
Chirophobia — Fear of hands
Cholerophobia — Fear of anger or Cholera
Chorophobia — Fear of dancing
Chrematophobia — Fear of money
Chromatophobia — Fear of colors
Chronomentrophobia — Fear of clocks
Chronophobia — Fear of time
Claustrophobia — Fear of confined or small spaces
Cleisiophobia — Fear of being locked in an enclosed place
Cleithrophobia — Fear of being enclosed
Cleptophobia — Fear of stealing
Climacophobia — Fear of stairs, climbing stairs, or falling down stairs
Clinophobia — Fear of going to bed
Cnidophobia — Fear of stings or being stung
Coimetrophobia — Fear of cemeteries
Coitophobia — Fear of coitus, sex, or sexual intercourse
Cometophobia — Fear of comets
Coprastasophobia — Fear of constipation
Coprophobia — Fear of feces and fecal matter
Coulrophobia — Fear of clowns
Counterphobia — Fear of The preference by a phobic for fearful situations
Cremnophobia — Fear of precipices
Cryophobia — Fear of extreme cold, ice, or frost
Crystallophobia — Fear of crystals or glass
Cyberphobia — Fear of computers or working on a computer
Cyclophobia — Fear of bicycles
Cymophobia — Fear of waves or wave-like motion
Cynophobia — Fear of dogs, canines, or rabies
Cyprianophobia — Fear of prostitutes, venereal disease, or STDs
The Phobia List: D
Daemonophobia — Fear of demons or daemons
Decidophobia — Fear of making decisions
Defecaloesiophobia — Fear of painful bowels movements
Deipnophobia — Fear of dining or dinner conversation
Demophobia — Fear of crowds
Dendrophobia — Fear of trees
Dentophobia — Fear of dentists
Dermatopathophobia — Fear of skin disease or skin lesions
Dextrophobia — Fear of objects at the right side of the body
Diabetophobia — Fear of diabetes
Didaskaleinophobia — Fear of going to school
Dikephobia — Fear of justice
Dinophobia — Fear of dizziness or whirlpools
Diplophobia — Fear of double vision
Dipsophobia — Fear of drinking
Dishabiliophobia — Fear of undressing in front of someone
Doraphobia — Fear of fur or skins of animals
Doxophobia — Fear of expressing opinions or of receiving praise
Driving Phobia — Fear of driving a motorized vehicle
Dromophobia — Fear of crossing streets
Dutchphobia — Fear of the Netherlands, the Dutch, Dutch Culture
Dysmorphophobia — Fear of deformity
Dystychiphobia — Fear of accidents
The Phobia List: E
Earthquakophobia — Fear of earthquakes
Ecclesiophobia — Fear of churchs
Eisoptrophobia — Fear of mirrors or of seeing oneself in a mirror
Electrophobia — Fear of electricity
Eleutherophobia — Fear of freedom
Emetophobia — Fear of vomiting or throwing up
Enetophobia — Fear of pins
Enissophobia — Fear of having committed an unpardonable sin or criticism
Entomophobia — Fear of insects or bugs
Eosophobia — Fear of dawn or daylight
Ephebiphobia — Fear of teenagers
Epistaxiophobia — Fear of nosebleeds
Epistemophobia — Fear of knowledge
Equinophobia — Fear of horses
Eremophobia — Fear of being oneself or lonliness
Ereuthophobia — Fear of redlights, blushing, or the color red
Ergasiophobia — Fear of work, functioning, or Surgeon's operating
Ergophobia — Fear of work
Erotophobia — Fear of sexual love or sexual questions
Euphobia — Fear of hearing good news
The Phobia List: F
Francophobia — Fear of France, French people, or French culture
Frigophobia — Fear of cold or cold things
The Phobia List: G
Gamophobia — Fear of marriage
Geliophobia — Fear of laughter
Geniophobia — Fear of chins
Genuphobia — Fear of knees
Gephydrophobia — Fear of crossing bridges
Gerascophobia — Fear of growing old or old people
Germanophobia — Fear of Germany, German People, or German culture
Geumaphobia — Fear of taste
Globophobia — Fear of balloons
Glossophobia — Fear of speaking in public or trying to speak
Graphophobia — Fear of writing or handwriting
Gymnophobia — Fear of nudity
Gynephobia — Fear of women
The Phobia List: H
Hadephobia — Fear of hell
Hagiophobia — Fear of saints or holy things
Harpaxophobia — Fear of being robbed
Hedonophobia — Fear of feeling pleasure
Heliophobia — Fear of the sun
Hellenologophobia — Fear of Greek terms or complex scientific terminology
Helminthophobia — Fear of being infested with worms
Hemaphobia — Fear of blood
Hereiophobia — Fear of challenges to official doctrine or of radical deviation
Herpetophobia — Fear of reptiles or creepy, crawly things
Heterophobia — Fear of the opposite sex
Hierophobia — Fear of priests or sacred things
Hippopotomonstrosesquippedaliophobia — Fear of long words
Hobophobia — Fear of bums or beggars
Hodophobia — Fear of road travel
Homichlophobia — Fear of fog
Homilophobia — Fear of sermons
Homophobia — Fear of sameness, monotony, homosexuality, or becoming homosexual
Hoplophobia — Fear of firearms
Hormephobia — Fear of shock
Hyalophobia — Fear of glass
Hydrargyophobia — Fear of mercurial medicines
Hydrophobia — Fear of water
Hydrophobophobia — Fear of rabies
Hygrophobia — Fear of liquids, dampness, or moisture
Hylephobia — Fear of materialism or epilepsy
Hypegiaphobia — Fear of responsibility
Hypnophobia — Fear of sleep or being hypnotized
The Phobia List: I
Iatrophobia — Fear of doctors or going to the doctor
Ichthyophobia — Fear of fish
Ideophobia — Fear of ideas
Illyngophobia — Fear of vertigo or feeling dizzy when looking down
Insomnia — Fear of Inability to Sleep
Iophobia — Fear of poison
Isopterophobia — Fear of termites, insects that eat wood
The Phobia List: J
Japanophobia — Fear of Japanese
Judeophobia — Fear of Jewish People
The Phobia List: K
Kakorrhaphiophobia — Fear of failure or defeat
Kenophobia — Fear of voids or empty spaces
Kinesophobia — Fear of movement or motion
Koinoniphobia — Fear of rooms
Kolpophobia — Fear of genitals, particularly female
Kopophobia — Fear of fatigue
Kosmikophobia — Fear of cosmic phenomenon
Kyphophobia — Fear of stooping
The Phobia List: L
Lachanophobia — Fear of vegetables
Lalophobia — Fear of speaking
Lepraphobia — Fear of leprosy
Leukophobia — Fear of the color white
Levophobia — Fear of things to the left side of the body
Ligyrophobia — Fear of loud noises
Lilapsophobia — Fear of tornado or hurricanes
Limnophobia — Fear of lakes
Linonophobia — Fear of string
Liticaphobia — Fear of lawsuits
Lockiophobia — Fear of childbirth
Logizomechanophobia — Fear of computers
Logophobia — Fear of words
Luiphobia — Fear of lues or syphillis
Lutraphobia — Fear of otters
The Phobia List: M
Macrophobia — Fear of long waits
Mageirocophobia — Fear of cooking
Malaxophobia — Fear of love play
Maniaphobia — Fear of insanity
Mastigophobia — Fear of punishment
Mechanophobia — Fear of machines
Medomalacuphobia — Fear of losing an erection
Medorthophobia — Fear of an erect penis
Megalophobia — Fear of large things
Melanophobia — Fear of the color black
Melophobia — Fear of music
Meningitophobia — Fear of brain disease
Menophobia — Fear of menstruation
Merinthophobia — Fear of being bound or tied up
Metallophobia — Fear of metal
Metathesiophobia — Fear of changes
Meteorophobia — Fear of meteors
Metrophobia — Fear of poetry
Microbiophobia — Fear of microbes
Microphobia — Fear of small things
Misophobia — Fear of being contaminated with dirt or germs
Mnemophobia — Fear of memories
Monopathophobia — Fear of definite disease
Motorphobia — Fear of automobiles
Mottephobia — Fear of moths
Murophobia — Fear of mice
Mycophobia — Fear of mushrooms
Myrmecophobia — Fear of ants
Mythophobia — Fear of myths, stories, or false statements
The Phobia List: N
Narcissistic Personality Disorder — Fear of -
Necrophobia — Fear of death or dead things
Neopharmaphobia — Fear of new drugs
Nephophobia — Fear of clouds
Noctiphobia — Fear of the night
Nomatophobia — Fear of names
Nosocomephobia — Fear of hospitals
Nosophobia — Fear of becoming ill
Nostophobia — Fear of returning home
Novercaphobia — Fear of your step-mother
Nucleomituphobia — Fear of nuclear weapons
Nudophobia — Fear of nudity or nakedness
Nyctohylophobia — Fear of dark wooded areas or forests at night
The Phobia List: O
Obesophobia — Fear of gaining weight
Ochlophobia — Fear of crowds or mobs
Ochophobia — Fear of vehicles
Octophobia — Fear of the figure 8
Odontophobia — Fear of teeth or dental surgery
Oenophobia — Fear of wines
Oikophobia — Fear of houses, home surroundings, or being in a house
Olfactophobia — Fear of smells
Ombrophobia — Fear of rain or of being rained on
Ommatophobia — Fear of eyes
Oneirogmophobia — Fear of wet dreams
Oneirophobia — Fear of dreams
Onomatophobia — Fear of hearing a certain word or of names
Ophidiophobia — Fear of snakes
Ophthalmophobia — Fear of being stared at
Opiophobia — Fear of Fear of medical doctors experience of prescribing needed pain medications for patients
Optophobia — Fear of opening one's eyes
Ornithophobia — Fear of birds
Orthophobia — Fear of property
Ostraconophobia — Fear of shellfish
Ouranophobia — Fear of heaven
The Phobia List: P
Pagophobia — Fear of ice or frost
Panophobia — Fear of everything
Panthophobia — Fear of suffering or disease
Papaphobia — Fear of the Pope
Papyrophobia — Fear of paper
Paralipophobia — Fear of neglecting duty or neglecting responsibility
Paraphobia — Fear of sexual perversion
Parasitophobia — Fear of parasites
Paraskavedekatriaphobia — Fear of Friday the 13th
Parthenophobia — Fear of virgins or young girls
Pathophobia — Fear of disease
Patroiophobia — Fear of heredity
Peccatophobia — Fear of sinning
Pediculophobia — Fear of lice
Pediophobia — Fear of dolls
Pedophobia — Fear of children
Peladophobia — Fear of bald people
Pellagrophobia — Fear of pellagra
Peniaphobia — Fear of poverty
Pentheraphobia — Fear of mother-in-law
Phagophobia — Fear of swallowing or eating
Phalacrophobia — Fear of becoming bald
Pharmacophobia — Fear of taking medicine or drugs
Phengophobia — Fear of daylight or sunshine
Philemaphobia — Fear of kissing
Philophobia — Fear of falling in love or being in love
Philosophobia — Fear of philosophy
Phobophobia — Fear of phobias
Phonophobia — Fear of noises, voices, one's own voice, or telephones
Photoaugliaphobia — Fear of glaring lights
Photophobia — Fear of light
Phronemophobia — Fear of thinking
Phthisiophobia — Fear of tuberculosis
Placophobia — Fear of tombstones
Plutophobia — Fear of wealth
Pneumatiphobia — Fear of spirits
Pnigerophobia — Fear of choking of being smothered
Pogonophobia — Fear of beards
Poliosophobia — Fear of contracting poliomyelitis
Politicophobia — Fear of politicians
Polyphobia — Fear of many things
Ponophobia — Fear of overworking or of pain
Porphyrophobia — Fear of the color purple
Potamophobia — Fear of rivers or running water
Potophobia — Fear of alcohol
Proctophobia — Fear of rectums
Prosophobia — Fear of progress
Psellismophobia — Fear of stuttering
Psychophobia — Fear of the mind
Psychrophobia — Fear of the cold
Pteromerhanophobia — Fear of flying
Pteronophobia — Fear of being tickled by feathers
Pupaphobia — Fear of puppets
Pyrexiophobia — Fear of fever
The Phobia List: R
Radiophobia — Fear of radiation or x-rays
Ranidaphobia — Fear of frogs
Rectophobia — Fear of rectums or rectal diseases
Rhabdophobia — Fear of being severely punished, beaten by a rod, or severely criticized
Rhypophobia — Fear of defecation
Rhytiphobia — Fear of getting wrinkles
Rupophobia — Fear of dirt
Russophobia — Fear of Russians
The Phobia List: S
Samhainophobia — Fear of Halloween
Satanophobia — Fear of Satan or The Devil
Scabiophobia — Fear of scabies
Scelerophibia — Fear of bad men or burglars
Sciaphobia — Fear of shadows
Scoleciphobia — Fear of worms
Scolionophobia — Fear of school
Scopophobia — Fear of being seen or stared at
Scoptophobia — Fear of blindness in visual field
Scriptophobia — Fear of writing in public
Selachophobia — Fear of sharks
Selaphobia — Fear of light flashes
Selenophobia — Fear of the moon
Seplophobia — Fear of decaying matter
Siderodromophobia — Fear of trains, railroads, or train travel
Siderophobia — Fear of stars
Sinistrophobia — Fear of things to the left or left-handed
Sinophobia — Fear of China, Chinese, or Chinese culture
Sitiophobia — Fear of food or eating
Soceraphobia — Fear of parents-in-law
Social Phobia — Fear of social situations
Sociophobia — Fear of society or people in general
Somniphobia — Fear of sleep
Sophophobia — Fear of learning
Soteriophobia — Fear of dependence on others
Spacephobia — Fear of outer space
Spectrophobia — Fear of specters or ghosts
Spheksophobia — Fear of wasps
Stasibasiphobia — Fear of standing or walking
Statue Phobia — Fear of statues or effigies
Staurophobia — Fear of crosses or the crucifix
Stenophobia — Fear of narrow things or places
Symbolophobia — Fear of symbolism
Symmetrophobia — Fear of symmetry
Syngenesophobia — Fear of relatives
The Phobia List: T
Tachophobia — Fear of speed
Taeniophobia — Fear of tapeworms
Taphephobia — Fear of being buried alive or cemeteries
Tapinophobia — Fear of being contagious
Taurophobia — Fear of bulls
Technophobia — Fear of technology or computers
Teleophobia — Fear of definite plans or Religious ceremony
Telephonophobia — Fear of telephones
Teratophobia — Fear of bearing a deformed child, monsters, or deformed people
Testophobia — Fear of taking tests
Tetanophobia — Fear of lockjaw or tetanus
Textophobia — Fear of certain fabrics
Thalassophobia — Fear of the sea or the ocean
Thanatophobia — Fear of death, dying, being buried, cremation, or entombment
Theatrophobia — Fear of theaters
Theologicophobia — Fear of theology
Theophobia — Fear of gods or religion
Thermophobia — Fear of heat
Tocophobia — Fear of pregnancy or childbirth
Tomophobia — Fear of surgery or surgical operations
Topophobia — Fear of fear of certain places or situations
Toxicophobia — Fear of poison or being accidently poisoned
Traumatophobia — Fear of injury or battle
Tremophobia — Fear of trembling
Trichinophobia — Fear of trichinosis
Trichopathophobia — Fear of hair
Triskaidekaphobia — Fear of the number 13
Tropophobia — Fear of moving or making changes
Trypanophobia — Fear of injections
Tyrannophobia — Fear of tyrants
The Phobia List: U
Urophobia — Fear of urine or urinating
The Phobia List: V
Vaccinophobia — Fear of vaccination
Verminophobia — Fear of germs
Vestiphobia — Fear of clothing
Virginitiphobia — Fear of rape
Vitricophobia — Fear of step-father's
The Phobia List: W
Walloonphobia — Fear of the Walloons
Wiccaphobia — Fear of witches and witchcraft
The Phobia List: X
Xanthophobia — Fear of the color yellow or the word yellow
Xenoglossophobia — Fear of foreign languages
Xenophobia — Fear of strangers or foreigners
Xerophobia — Fear of dryness
Xylophobia — Fear of wood, wooden objects, or forests
Xyrophobia — Fear of razors
The Phobia List: Z
Zelophobia — Fear of jealousy
Zemmiphobia — Fear of the great mole rat
Zeusophobia — Fear of God or gods
Zoophobia — Fear of animals
Although there are many hundreds of 'different' phobias, all phobias are in fact very similar: a particular stimulus, be it spiders, snakes, or pretty well anything else triggering the phobic individuals fear response when it isn't appropriate.
The Phobia List: A
Ablutophobia — Fear of washing, bathing, or cleaning
Acarophobia — Fear of itching or the insects that cause itching
Acerophobia — Fear of sourness or things that are sour
Achluophobia — Fear of darkness or the dark
Acousticophobia — Fear of noise or sound
Acrophobia — Fear of heights or high levels
Aeroacrophobia — Fear of open high places
Aeronausiphobia — Fear of vomiting secondary to airsickness
Aerophobia — Fear of draft, swallowing air, or airbourne noxious substances
Agateophobia — Fear of insanity or becoming insane
Agliophobia — Fear of pain
Agoraphobia — Fear of open spaces, leaving a safe place, or crowded public places
Agraphobia — Fear of sexual abuse
Agrizoophobia — Fear of wild animals
Agyrophobia — Fear of streets or crossing the street
Aichmophobia — Fear of needles, pins, or pointed objects
Ailurophobia — Fear of cats
Albuminurophobia — Fear of kidney disease
Alektorophobia — Fear of chickens
Algophobia — Fear of garlic
Alliumphobia — Fear of opinions or beliefs
Altophobia — Fear of dust
Amathophobia — Fear of riding in cars
Amaxophobia — Fear of walking
Amnesiphobia — Fear of amnesia
Amychophobia — Fear of scratches or being scratched
Anablephobia — Fear of looking up
Androphobia — Fear of men
Anemophobia — Fear of wind or air drafts
Anginophobia — Fear of angina, choking, or narrowness
Anglophobia — Fear of England, English Culture, or English People
Angrophobia — Fear of anger or becoming angry
Ankylophobia — Fear of immobility of a joint
Anthophobia — Fear of flowers
Anthropophobia — Fear of people or society
Antlophobia — Fear of floods
Anuptaphobia — Fear of staying single
Anxiety — Fear of Anxiety
Apeirophobia — Fear of infinity
Aphenphosmphobia — Fear of being touched
Apiphobia — Fear of bees
Apotemnophobia — Fear of persons with amputations
Arachibutyrophobia — Fear of peanut butter sticking to the roof of the mouth
Arachnephobia — Fear of spiders
Arithmophobia — Fear of numbers
Arsonphobia — Fear of fire or flames
Asthenophobia — Fear of fainting or weakness
Astraphobia — Fear of thunder and lightning
Astrophobia — Fear of stars and celestial space
Asymmetriphobia — Fear of asymmetrical things
Ataxiophobia — Fear of ataxia (muscular incoordination)
Ataxophobia — Fear of disorder or untidiness
Atelophobia — Fear of imperfection
Atephobia — Fear of ruin or ruins
Athazagoraphobia — Fear of being forgotton, being ignored, or forgetting
Atomosophobia — Fear of atomic explosions
Atychiphobia — Fear of failure
Aulophobia — Fear of flutes
Aurophobia — Fear of gold
Auroraphobia — Fear of Northern lights
Autodysomophobia — Fear of one that has a vile odor
Automatonophobia — Fear of ventriloquist's dummies, animatronic creatures or wax statues
Automysophobia — Fear of being dirty
Autophobia — Fear of solitude, being alone, oneself, or being by oneself
Aviophobia — Fear of flying
The Phobia List: B
Bacillophobia — Fear of microbes
Bacteriophobia — Fear of bacteria
Ballistophobia — Fear of missiles or bullets
Barophobia — Fear of gravity
Basiphobia — Fear of inability to stand or falling
Bathmophobia — Fear of stairs or steep slopes
Bathophobia — Fear of depth
Batophobia — Fear of heights or being close to high buildings
Batrachophobia — Fear of amphibians, frogs, newts, or salamanders
Bibliophobia — Fear of books
Blennophobia — Fear of slime
Body Dysmorphic Disorder — Fear of having ugly or unattractive features
Bogyphobia — Fear of bogies or the bogeyman
Bolshephobia — Fear of Bolsheviks
Botanophobia — Fear of plants
Bromidrophobia — Fear of bodily odor or bodily smell
Bufonophobia — Fear of toads
The Phobia List: C
Cacophobia — Fear of ugliness or things that are ugly
Cainophobia — Fear of newness or novelty
Caligynephobia — Fear of beautiful women
Cancerophobia — Fear of cancer
Cardiophobia — Fear of the heart
Carnophobia — Fear of meat
Catagelophobia — Fear of being ridiculed or ridicule
Catapedaphobia — Fear of jumping from high and low places
Cathisophobia — Fear of sitting
Catoptrophobia — Fear of mirrors
Cheimaphobia — Fear of cold
Chemophobia — Fear of chemicals or working with chemicals
Cherophobia — Fear of gaiety
Chionophobia — Fear of snow
Chirophobia — Fear of hands
Cholerophobia — Fear of anger or Cholera
Chorophobia — Fear of dancing
Chrematophobia — Fear of money
Chromatophobia — Fear of colors
Chronomentrophobia — Fear of clocks
Chronophobia — Fear of time
Claustrophobia — Fear of confined or small spaces
Cleisiophobia — Fear of being locked in an enclosed place
Cleithrophobia — Fear of being enclosed
Cleptophobia — Fear of stealing
Climacophobia — Fear of stairs, climbing stairs, or falling down stairs
Clinophobia — Fear of going to bed
Cnidophobia — Fear of stings or being stung
Coimetrophobia — Fear of cemeteries
Coitophobia — Fear of coitus, sex, or sexual intercourse
Cometophobia — Fear of comets
Coprastasophobia — Fear of constipation
Coprophobia — Fear of feces and fecal matter
Coulrophobia — Fear of clowns
Counterphobia — Fear of The preference by a phobic for fearful situations
Cremnophobia — Fear of precipices
Cryophobia — Fear of extreme cold, ice, or frost
Crystallophobia — Fear of crystals or glass
Cyberphobia — Fear of computers or working on a computer
Cyclophobia — Fear of bicycles
Cymophobia — Fear of waves or wave-like motion
Cynophobia — Fear of dogs, canines, or rabies
Cyprianophobia — Fear of prostitutes, venereal disease, or STDs
The Phobia List: D
Daemonophobia — Fear of demons or daemons
Decidophobia — Fear of making decisions
Defecaloesiophobia — Fear of painful bowels movements
Deipnophobia — Fear of dining or dinner conversation
Demophobia — Fear of crowds
Dendrophobia — Fear of trees
Dentophobia — Fear of dentists
Dermatopathophobia — Fear of skin disease or skin lesions
Dextrophobia — Fear of objects at the right side of the body
Diabetophobia — Fear of diabetes
Didaskaleinophobia — Fear of going to school
Dikephobia — Fear of justice
Dinophobia — Fear of dizziness or whirlpools
Diplophobia — Fear of double vision
Dipsophobia — Fear of drinking
Dishabiliophobia — Fear of undressing in front of someone
Doraphobia — Fear of fur or skins of animals
Doxophobia — Fear of expressing opinions or of receiving praise
Driving Phobia — Fear of driving a motorized vehicle
Dromophobia — Fear of crossing streets
Dutchphobia — Fear of the Netherlands, the Dutch, Dutch Culture
Dysmorphophobia — Fear of deformity
Dystychiphobia — Fear of accidents
The Phobia List: E
Earthquakophobia — Fear of earthquakes
Ecclesiophobia — Fear of churchs
Eisoptrophobia — Fear of mirrors or of seeing oneself in a mirror
Electrophobia — Fear of electricity
Eleutherophobia — Fear of freedom
Emetophobia — Fear of vomiting or throwing up
Enetophobia — Fear of pins
Enissophobia — Fear of having committed an unpardonable sin or criticism
Entomophobia — Fear of insects or bugs
Eosophobia — Fear of dawn or daylight
Ephebiphobia — Fear of teenagers
Epistaxiophobia — Fear of nosebleeds
Epistemophobia — Fear of knowledge
Equinophobia — Fear of horses
Eremophobia — Fear of being oneself or lonliness
Ereuthophobia — Fear of redlights, blushing, or the color red
Ergasiophobia — Fear of work, functioning, or Surgeon's operating
Ergophobia — Fear of work
Erotophobia — Fear of sexual love or sexual questions
Euphobia — Fear of hearing good news
The Phobia List: F
Francophobia — Fear of France, French people, or French culture
Frigophobia — Fear of cold or cold things
The Phobia List: G
Gamophobia — Fear of marriage
Geliophobia — Fear of laughter
Geniophobia — Fear of chins
Genuphobia — Fear of knees
Gephydrophobia — Fear of crossing bridges
Gerascophobia — Fear of growing old or old people
Germanophobia — Fear of Germany, German People, or German culture
Geumaphobia — Fear of taste
Globophobia — Fear of balloons
Glossophobia — Fear of speaking in public or trying to speak
Graphophobia — Fear of writing or handwriting
Gymnophobia — Fear of nudity
Gynephobia — Fear of women
The Phobia List: H
Hadephobia — Fear of hell
Hagiophobia — Fear of saints or holy things
Harpaxophobia — Fear of being robbed
Hedonophobia — Fear of feeling pleasure
Heliophobia — Fear of the sun
Hellenologophobia — Fear of Greek terms or complex scientific terminology
Helminthophobia — Fear of being infested with worms
Hemaphobia — Fear of blood
Hereiophobia — Fear of challenges to official doctrine or of radical deviation
Herpetophobia — Fear of reptiles or creepy, crawly things
Heterophobia — Fear of the opposite sex
Hierophobia — Fear of priests or sacred things
Hippopotomonstrosesquippedaliophobia — Fear of long words
Hobophobia — Fear of bums or beggars
Hodophobia — Fear of road travel
Homichlophobia — Fear of fog
Homilophobia — Fear of sermons
Homophobia — Fear of sameness, monotony, homosexuality, or becoming homosexual
Hoplophobia — Fear of firearms
Hormephobia — Fear of shock
Hyalophobia — Fear of glass
Hydrargyophobia — Fear of mercurial medicines
Hydrophobia — Fear of water
Hydrophobophobia — Fear of rabies
Hygrophobia — Fear of liquids, dampness, or moisture
Hylephobia — Fear of materialism or epilepsy
Hypegiaphobia — Fear of responsibility
Hypnophobia — Fear of sleep or being hypnotized
The Phobia List: I
Iatrophobia — Fear of doctors or going to the doctor
Ichthyophobia — Fear of fish
Ideophobia — Fear of ideas
Illyngophobia — Fear of vertigo or feeling dizzy when looking down
Insomnia — Fear of Inability to Sleep
Iophobia — Fear of poison
Isopterophobia — Fear of termites, insects that eat wood
The Phobia List: J
Japanophobia — Fear of Japanese
Judeophobia — Fear of Jewish People
The Phobia List: K
Kakorrhaphiophobia — Fear of failure or defeat
Kenophobia — Fear of voids or empty spaces
Kinesophobia — Fear of movement or motion
Koinoniphobia — Fear of rooms
Kolpophobia — Fear of genitals, particularly female
Kopophobia — Fear of fatigue
Kosmikophobia — Fear of cosmic phenomenon
Kyphophobia — Fear of stooping
The Phobia List: L
Lachanophobia — Fear of vegetables
Lalophobia — Fear of speaking
Lepraphobia — Fear of leprosy
Leukophobia — Fear of the color white
Levophobia — Fear of things to the left side of the body
Ligyrophobia — Fear of loud noises
Lilapsophobia — Fear of tornado or hurricanes
Limnophobia — Fear of lakes
Linonophobia — Fear of string
Liticaphobia — Fear of lawsuits
Lockiophobia — Fear of childbirth
Logizomechanophobia — Fear of computers
Logophobia — Fear of words
Luiphobia — Fear of lues or syphillis
Lutraphobia — Fear of otters
The Phobia List: M
Macrophobia — Fear of long waits
Mageirocophobia — Fear of cooking
Malaxophobia — Fear of love play
Maniaphobia — Fear of insanity
Mastigophobia — Fear of punishment
Mechanophobia — Fear of machines
Medomalacuphobia — Fear of losing an erection
Medorthophobia — Fear of an erect penis
Megalophobia — Fear of large things
Melanophobia — Fear of the color black
Melophobia — Fear of music
Meningitophobia — Fear of brain disease
Menophobia — Fear of menstruation
Merinthophobia — Fear of being bound or tied up
Metallophobia — Fear of metal
Metathesiophobia — Fear of changes
Meteorophobia — Fear of meteors
Metrophobia — Fear of poetry
Microbiophobia — Fear of microbes
Microphobia — Fear of small things
Misophobia — Fear of being contaminated with dirt or germs
Mnemophobia — Fear of memories
Monopathophobia — Fear of definite disease
Motorphobia — Fear of automobiles
Mottephobia — Fear of moths
Murophobia — Fear of mice
Mycophobia — Fear of mushrooms
Myrmecophobia — Fear of ants
Mythophobia — Fear of myths, stories, or false statements
The Phobia List: N
Narcissistic Personality Disorder — Fear of -
Necrophobia — Fear of death or dead things
Neopharmaphobia — Fear of new drugs
Nephophobia — Fear of clouds
Noctiphobia — Fear of the night
Nomatophobia — Fear of names
Nosocomephobia — Fear of hospitals
Nosophobia — Fear of becoming ill
Nostophobia — Fear of returning home
Novercaphobia — Fear of your step-mother
Nucleomituphobia — Fear of nuclear weapons
Nudophobia — Fear of nudity or nakedness
Nyctohylophobia — Fear of dark wooded areas or forests at night
The Phobia List: O
Obesophobia — Fear of gaining weight
Ochlophobia — Fear of crowds or mobs
Ochophobia — Fear of vehicles
Octophobia — Fear of the figure 8
Odontophobia — Fear of teeth or dental surgery
Oenophobia — Fear of wines
Oikophobia — Fear of houses, home surroundings, or being in a house
Olfactophobia — Fear of smells
Ombrophobia — Fear of rain or of being rained on
Ommatophobia — Fear of eyes
Oneirogmophobia — Fear of wet dreams
Oneirophobia — Fear of dreams
Onomatophobia — Fear of hearing a certain word or of names
Ophidiophobia — Fear of snakes
Ophthalmophobia — Fear of being stared at
Opiophobia — Fear of Fear of medical doctors experience of prescribing needed pain medications for patients
Optophobia — Fear of opening one's eyes
Ornithophobia — Fear of birds
Orthophobia — Fear of property
Ostraconophobia — Fear of shellfish
Ouranophobia — Fear of heaven
The Phobia List: P
Pagophobia — Fear of ice or frost
Panophobia — Fear of everything
Panthophobia — Fear of suffering or disease
Papaphobia — Fear of the Pope
Papyrophobia — Fear of paper
Paralipophobia — Fear of neglecting duty or neglecting responsibility
Paraphobia — Fear of sexual perversion
Parasitophobia — Fear of parasites
Paraskavedekatriaphobia — Fear of Friday the 13th
Parthenophobia — Fear of virgins or young girls
Pathophobia — Fear of disease
Patroiophobia — Fear of heredity
Peccatophobia — Fear of sinning
Pediculophobia — Fear of lice
Pediophobia — Fear of dolls
Pedophobia — Fear of children
Peladophobia — Fear of bald people
Pellagrophobia — Fear of pellagra
Peniaphobia — Fear of poverty
Pentheraphobia — Fear of mother-in-law
Phagophobia — Fear of swallowing or eating
Phalacrophobia — Fear of becoming bald
Pharmacophobia — Fear of taking medicine or drugs
Phengophobia — Fear of daylight or sunshine
Philemaphobia — Fear of kissing
Philophobia — Fear of falling in love or being in love
Philosophobia — Fear of philosophy
Phobophobia — Fear of phobias
Phonophobia — Fear of noises, voices, one's own voice, or telephones
Photoaugliaphobia — Fear of glaring lights
Photophobia — Fear of light
Phronemophobia — Fear of thinking
Phthisiophobia — Fear of tuberculosis
Placophobia — Fear of tombstones
Plutophobia — Fear of wealth
Pneumatiphobia — Fear of spirits
Pnigerophobia — Fear of choking of being smothered
Pogonophobia — Fear of beards
Poliosophobia — Fear of contracting poliomyelitis
Politicophobia — Fear of politicians
Polyphobia — Fear of many things
Ponophobia — Fear of overworking or of pain
Porphyrophobia — Fear of the color purple
Potamophobia — Fear of rivers or running water
Potophobia — Fear of alcohol
Proctophobia — Fear of rectums
Prosophobia — Fear of progress
Psellismophobia — Fear of stuttering
Psychophobia — Fear of the mind
Psychrophobia — Fear of the cold
Pteromerhanophobia — Fear of flying
Pteronophobia — Fear of being tickled by feathers
Pupaphobia — Fear of puppets
Pyrexiophobia — Fear of fever
The Phobia List: R
Radiophobia — Fear of radiation or x-rays
Ranidaphobia — Fear of frogs
Rectophobia — Fear of rectums or rectal diseases
Rhabdophobia — Fear of being severely punished, beaten by a rod, or severely criticized
Rhypophobia — Fear of defecation
Rhytiphobia — Fear of getting wrinkles
Rupophobia — Fear of dirt
Russophobia — Fear of Russians
The Phobia List: S
Samhainophobia — Fear of Halloween
Satanophobia — Fear of Satan or The Devil
Scabiophobia — Fear of scabies
Scelerophibia — Fear of bad men or burglars
Sciaphobia — Fear of shadows
Scoleciphobia — Fear of worms
Scolionophobia — Fear of school
Scopophobia — Fear of being seen or stared at
Scoptophobia — Fear of blindness in visual field
Scriptophobia — Fear of writing in public
Selachophobia — Fear of sharks
Selaphobia — Fear of light flashes
Selenophobia — Fear of the moon
Seplophobia — Fear of decaying matter
Siderodromophobia — Fear of trains, railroads, or train travel
Siderophobia — Fear of stars
Sinistrophobia — Fear of things to the left or left-handed
Sinophobia — Fear of China, Chinese, or Chinese culture
Sitiophobia — Fear of food or eating
Soceraphobia — Fear of parents-in-law
Social Phobia — Fear of social situations
Sociophobia — Fear of society or people in general
Somniphobia — Fear of sleep
Sophophobia — Fear of learning
Soteriophobia — Fear of dependence on others
Spacephobia — Fear of outer space
Spectrophobia — Fear of specters or ghosts
Spheksophobia — Fear of wasps
Stasibasiphobia — Fear of standing or walking
Statue Phobia — Fear of statues or effigies
Staurophobia — Fear of crosses or the crucifix
Stenophobia — Fear of narrow things or places
Symbolophobia — Fear of symbolism
Symmetrophobia — Fear of symmetry
Syngenesophobia — Fear of relatives
The Phobia List: T
Tachophobia — Fear of speed
Taeniophobia — Fear of tapeworms
Taphephobia — Fear of being buried alive or cemeteries
Tapinophobia — Fear of being contagious
Taurophobia — Fear of bulls
Technophobia — Fear of technology or computers
Teleophobia — Fear of definite plans or Religious ceremony
Telephonophobia — Fear of telephones
Teratophobia — Fear of bearing a deformed child, monsters, or deformed people
Testophobia — Fear of taking tests
Tetanophobia — Fear of lockjaw or tetanus
Textophobia — Fear of certain fabrics
Thalassophobia — Fear of the sea or the ocean
Thanatophobia — Fear of death, dying, being buried, cremation, or entombment
Theatrophobia — Fear of theaters
Theologicophobia — Fear of theology
Theophobia — Fear of gods or religion
Thermophobia — Fear of heat
Tocophobia — Fear of pregnancy or childbirth
Tomophobia — Fear of surgery or surgical operations
Topophobia — Fear of fear of certain places or situations
Toxicophobia — Fear of poison or being accidently poisoned
Traumatophobia — Fear of injury or battle
Tremophobia — Fear of trembling
Trichinophobia — Fear of trichinosis
Trichopathophobia — Fear of hair
Triskaidekaphobia — Fear of the number 13
Tropophobia — Fear of moving or making changes
Trypanophobia — Fear of injections
Tyrannophobia — Fear of tyrants
The Phobia List: U
Urophobia — Fear of urine or urinating
The Phobia List: V
Vaccinophobia — Fear of vaccination
Verminophobia — Fear of germs
Vestiphobia — Fear of clothing
Virginitiphobia — Fear of rape
Vitricophobia — Fear of step-father's
The Phobia List: W
Walloonphobia — Fear of the Walloons
Wiccaphobia — Fear of witches and witchcraft
The Phobia List: X
Xanthophobia — Fear of the color yellow or the word yellow
Xenoglossophobia — Fear of foreign languages
Xenophobia — Fear of strangers or foreigners
Xerophobia — Fear of dryness
Xylophobia — Fear of wood, wooden objects, or forests
Xyrophobia — Fear of razors
The Phobia List: Z
Zelophobia — Fear of jealousy
Zemmiphobia — Fear of the great mole rat
Zeusophobia — Fear of God or gods
Zoophobia — Fear of animals
Subscribe to:
Posts (Atom)